

Metastasis-free survival is associated with overall survival in men with PSA-recurrent prostate cancer treated with deferred androgen deprivation therapy
- PMID: 23946329
- PMCID: PMC3888237
- DOI: 10.1093/annonc/mdt335
Metastasis-free survival is associated with overall survival in men with PSA-recurrent prostate cancer treated with deferred androgen deprivation therapy
Abstract
Background: Clinical trials in men with biochemically recurrent prostate cancer (BRPC) have been hampered by long survival times, making overall survival (OS) a difficult end point to reach. Intermediate end points are needed in order to conduct such trials within a more feasible time frame.
Patients and methods: This is a retrospective analysis of 450 men with BRPC following prostatectomy treated at a single institution between 1981 and 2010, of which 140 developed subsequent metastases. Androgen deprivation therapy (ADT) was deferred until after the development of metastases. Cox regression models were developed to investigate factors influencing OS.
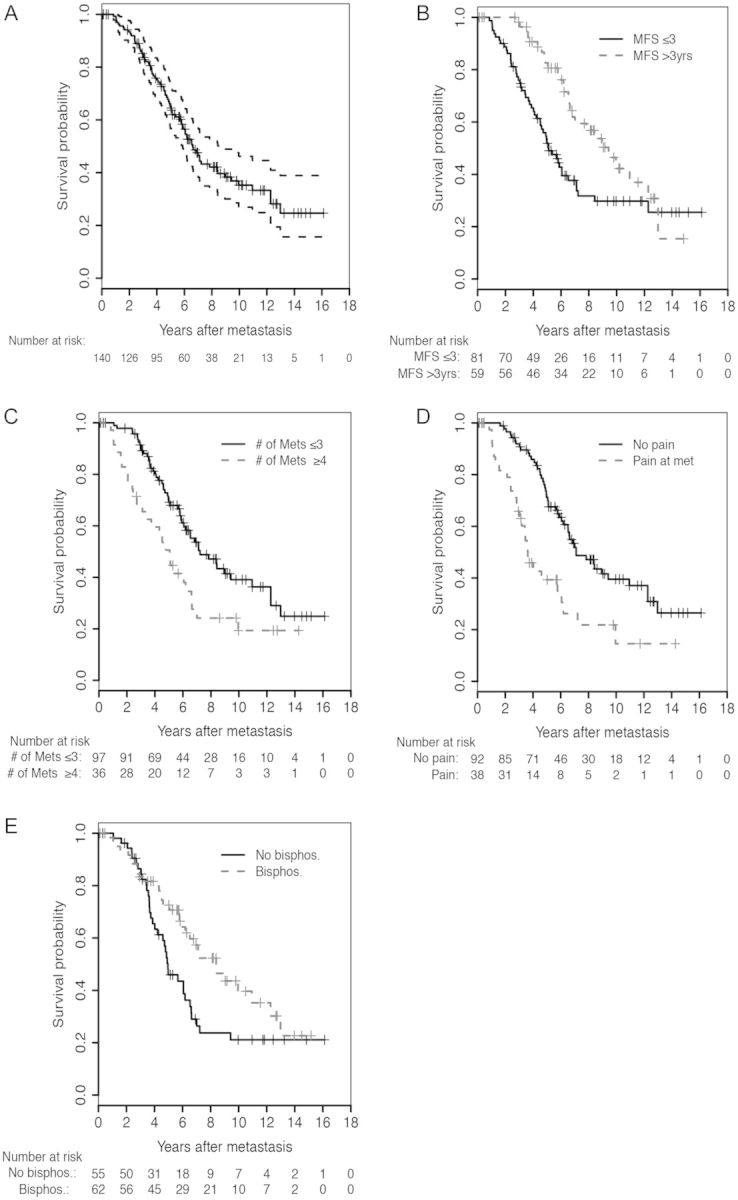
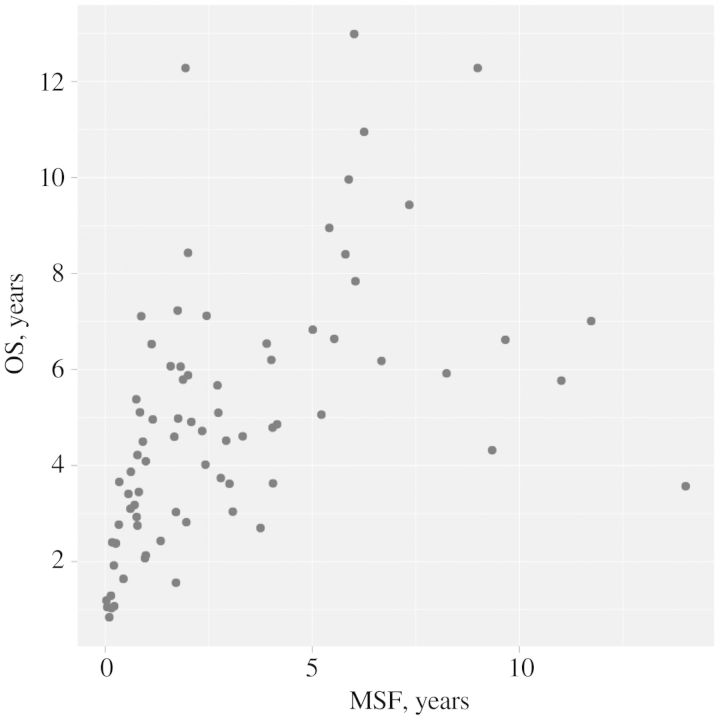
Results: Median metastasis-free survival (MFS) was 10.2 years [95% confidence interval (CI) 7.6-14.0 years]; median OS after metastasis was 6.6 years (95%CI 5.8-8.4 years). Multivariable Cox regressions identified four independently prognostic variables for OS: MFS (HR 0.77; 95% CI 0.63-0.94), number of metastases (≤3 versus ≥4; HR 0.50; 95% CI 0.29-0.85), pain (absent versus present; HR 0.43; 95% CI 0.25-0.72), and bisphosphonate use (yes versus no; HR 0.60; 95% CI 0.37-0.98).
Conclusions: MFS emerged as an independent predictor of OS in men with BRPC treated with deferred ADT after the development of metastases. MFS may be a reasonable intermediate end point in future clinical trials. This observation requires prospective validation.
Keywords: clinical trial end points; metastasis-free survival; prostate cancer.
Figures
Comment in
-
Prostate cancer: Intermediate efficacy end points to assess modern therapies.Nat Rev Urol. 2013 Dec;10(12):686-7. doi: 10.1038/nrurol.2013.269. Epub 2013 Nov 26. Nat Rev Urol. 2013. PMID: 24276080 Free PMC article.
References
-
- Siegel R, Naishadham D, Jemal A. Cancer statistics, 2012. CA Cancer J Clin. 2012;62:10–29. - PubMed
-
- Roehl KA, Han M, Ramos CG, et al. Cancer progression and survival rates following anatomical radical retropubic prostatectomy in 3,478 consecutive patients: long-term results. J Urol. 2004;172:910–914. - PubMed
-
- Pound CR, Partin AW, Eisenberger MA, et al. Natural history of progression after PSA elevation following radical prostatectomy. JAMA. 1999;281:1591–1597. - PubMed
-
- Sandler HM, Eisenberger MA. Assessing and treating patients with increasing prostate specific antigen following radical prostatectomy. J Urol. 2007;178:S20–S24. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
