

New ultrasound techniques for lymph node evaluation
- PMID: 23946589
- PMCID: PMC3740414
- DOI: 10.3748/wjg.v19.i30.4850
New ultrasound techniques for lymph node evaluation
Abstract
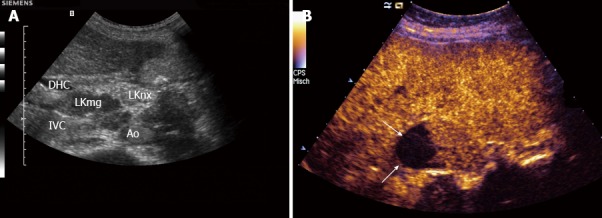
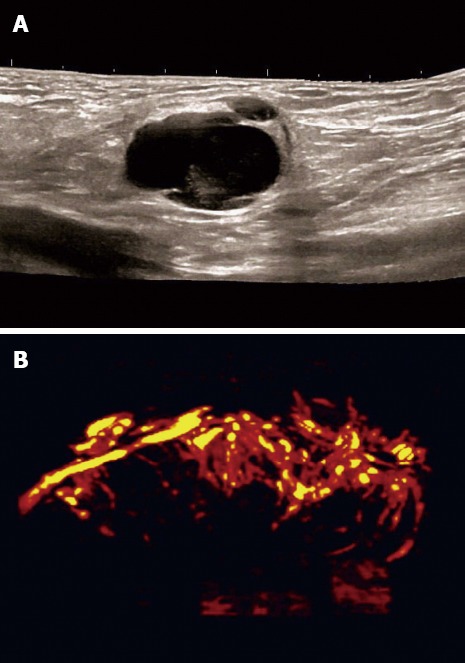
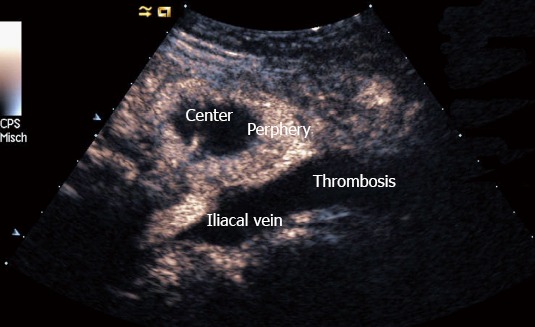
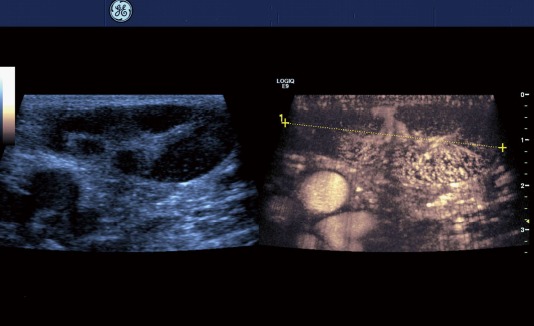
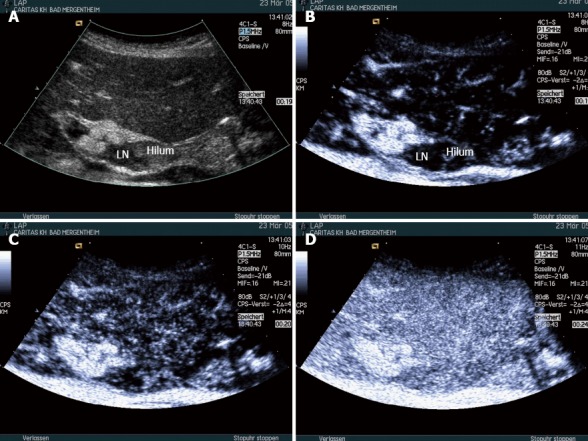
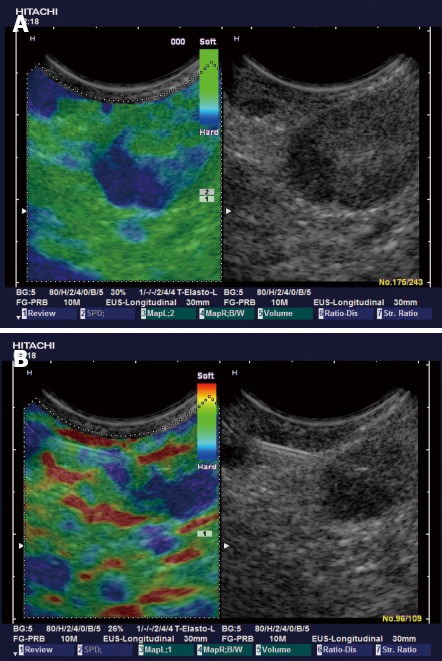
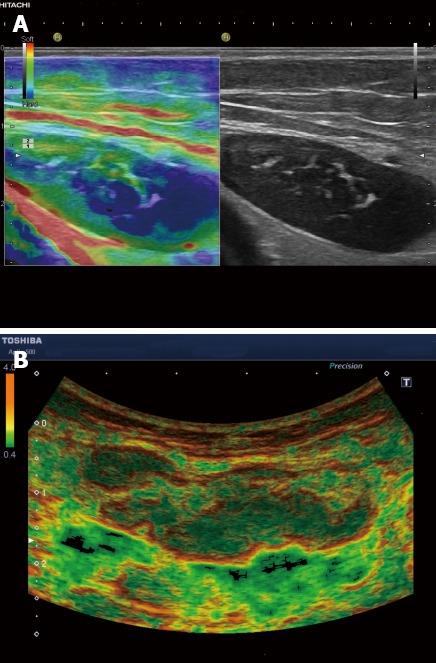
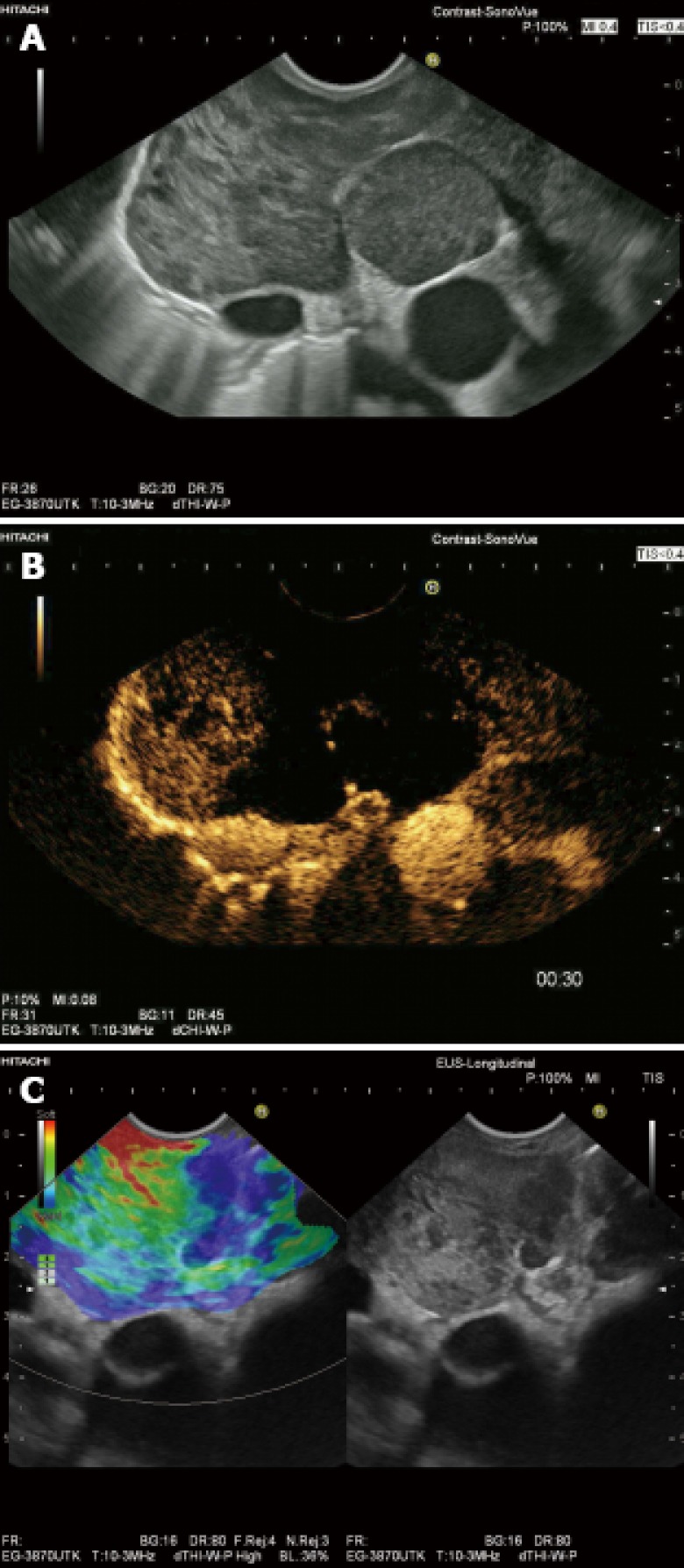
Conventional ultrasound (US) is the recommended imaging method for lymph node (LN) diseases with the advantages of high resolution, real time evaluation and relative low costs. Current indications of transcutaneous ultrasound and endoscopic ultrasound include the detection and characterization of lymph nodes and the guidance for LN biopsy. Recent advances in US technology, such as contrast enhanced ultrasound (CEUS), contrast enhanced endoscopic ultrasound (CE-EUS), and real time elastography show potential to improve the accuracy of US for the differential diagnosis of benign and malignant lymph nodes. In addition, CEUS and CE-EUS have been also used for the guidance of fine needle aspiration and assessment of treatment response. Complementary to size criteria, CEUS could also be used to evaluate response of tumor angiogenesis to anti-angiogenic therapies. In this paper we review current literature regarding evaluation of lymphadenopathy by new and innovative US techniques.
Keywords: Endoscopic ultrasound; Lymph node metastasis; Lymph nodes; Lymphoma; Ultrasound.
Figures
Similar articles
-
Endoscopic ultrasound elastography: Current status and future perspectives.World J Gastroenterol. 2015 Dec 21;21(47):13212-24. doi: 10.3748/wjg.v21.i47.13212. World J Gastroenterol. 2015. PMID: 26715804 Free PMC article. Review.
-
Endoscopic ultrasound-guided fine-needle aspiration and cytology for differentiating benign from malignant lymph nodes.Arab J Gastroenterol. 2017 Jun;18(2):74-79. doi: 10.1016/j.ajg.2017.05.015. Epub 2017 Jun 16. Arab J Gastroenterol. 2017. PMID: 28624157
-
A comparison of the accuracy of echo features during endoscopic ultrasound (EUS) and EUS-guided fine-needle aspiration for diagnosis of malignant lymph node invasion.Gastrointest Endosc. 1997 Jun;45(6):474-9. doi: 10.1016/s0016-5107(97)70176-7. Gastrointest Endosc. 1997. PMID: 9199903
-
[Clinical value of lymph node sonography].Praxis (Bern 1994). 2009 May 27;98(11):581-8. doi: 10.1024/1661-8157.98.11.581. Praxis (Bern 1994). 2009. PMID: 19472143 Review. German.
-
Performance of Endobronchial Ultrasound Elastography in the Differentiation of Malignant and Benign Mediastinal Lymph Nodes: Results in Real-life Practice.J Bronchology Interv Pulmonol. 2019 Jul;26(3):193-198. doi: 10.1097/LBR.0000000000000551. J Bronchology Interv Pulmonol. 2019. PMID: 30335666
Cited by
-
Correlation between physical characteristics of biopsy specimen and disease of cervical lymph node after contrast-enhanced ultrasound.BMC Surg. 2022 Jun 11;22(1):223. doi: 10.1186/s12893-022-01671-3. BMC Surg. 2022. PMID: 35690851 Free PMC article.
-
Chest wall - underappreciated structure in sonography. Part I: Examination methodology and ultrasound anatomy.J Ultrason. 2017 Sep;17(70):197-205. doi: 10.15557/JoU.2017.0029. Epub 2017 Sep 29. J Ultrason. 2017. PMID: 29075525 Free PMC article. Review.
-
Application of multimodal ultrasonography for differentiating benign and malignant cervical lymphadenopathy.Jpn J Radiol. 2021 Oct;39(10):938-945. doi: 10.1007/s11604-021-01131-7. Epub 2021 May 10. Jpn J Radiol. 2021. PMID: 33970452
-
Elastography of the Pancreas, Current View.Clin Endosc. 2019 Nov;52(6):533-540. doi: 10.5946/ce.2018.156. Epub 2019 Jul 17. Clin Endosc. 2019. PMID: 31311914 Free PMC article.
-
Application of conventional ultrasonography combined with contrast-enhanced ultrasonography in the axillary lymph nodes and evaluation of the efficacy of neoadjuvant chemotherapy in breast cancer patients.Br J Radiol. 2021 Sep 1;94(1125):20210520. doi: 10.1259/bjr.20210520. Br J Radiol. 2021. PMID: 34415197 Free PMC article.
References
-
- Sharma A, Fidias P, Hayman LA, Loomis SL, Taber KH, Aquino SL. Patterns of lymphadenopathy in thoracic malignancies. Radiographics. 2004;24:419–434. - PubMed
-
- Sumi M, Ohki M, Nakamura T. Comparison of sonography and CT for differentiating benign from malignant cervical lymph nodes in patients with squamous cell carcinoma of the head and neck. AJR Am J Roentgenol. 2001;176:1019–1024. - PubMed
-
- Hocke M, Menges M, Topalidis T, Dietrich CF, Stallmach A. Contrast-enhanced endoscopic ultrasound in discrimination between benign and malignant mediastinal and abdominal lymph nodes. J Cancer Res Clin Oncol. 2008;134:473–480. - PubMed
-
- Prenzel KL, Hölscher AH, Drebber U, Agavonova M, Gutschow CA, Bollschweiler E. Prognostic impact of nodal micrometastasis in early esophageal cancer. Eur J Surg Oncol. 2012;38:314–318. - PubMed
-
- Prenzel KL, Mönig SP, Sinning JM, Baldus SE, Brochhagen HG, Schneider PM, Hölscher AH. Lymph node size and metastatic infiltration in non-small cell lung cancer. Chest. 2003;123:463–467. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
