

Definition of compartment-based radical surgery in uterine cancer: modified radical hysterectomy in intermediate/high-risk endometrial cancer using peritoneal mesometrial resection (PMMR) by M Höckel translated to robotic surgery
- PMID: 23947937
- PMCID: PMC3751733
- DOI: 10.1186/1477-7819-11-198
Definition of compartment-based radical surgery in uterine cancer: modified radical hysterectomy in intermediate/high-risk endometrial cancer using peritoneal mesometrial resection (PMMR) by M Höckel translated to robotic surgery
Abstract
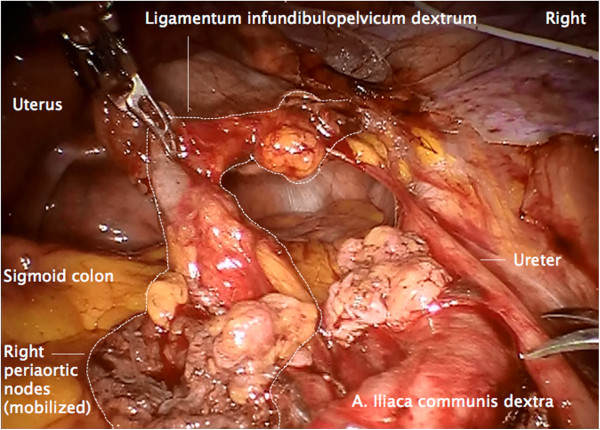
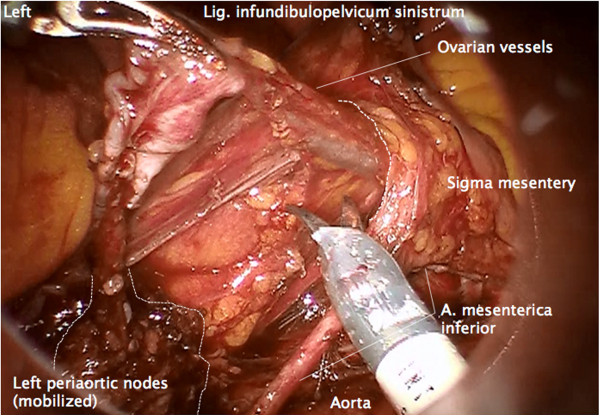
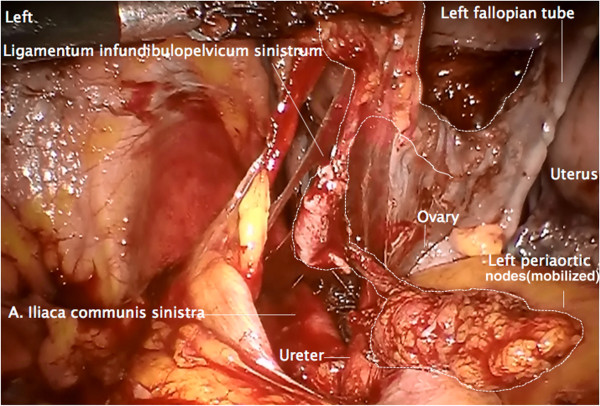
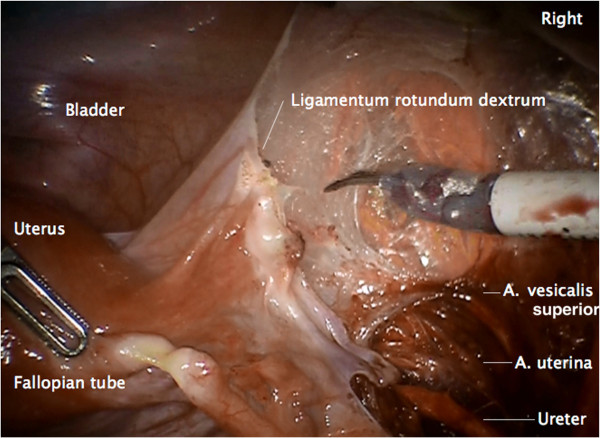
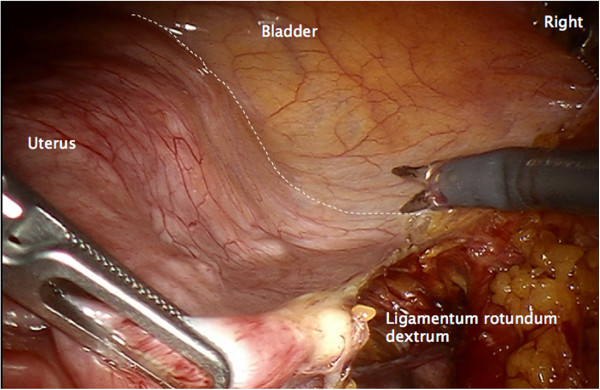
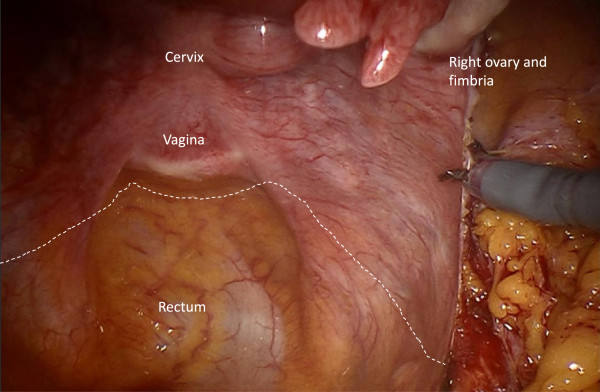
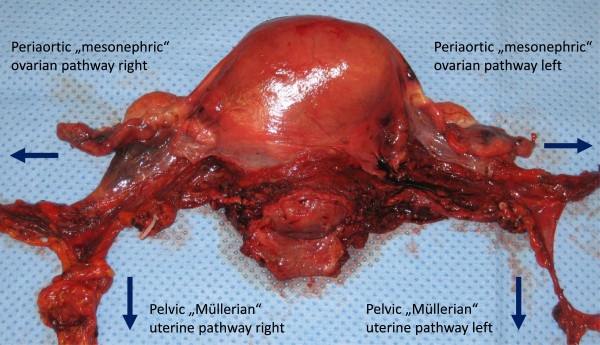
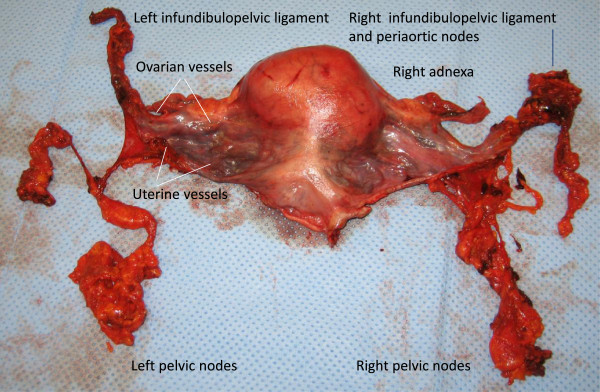
Background: The technique of compartment-based radical hysterectomy was originally described by M Höckel as total mesometrial resection (TMMR) for standard treatment of stage I and II cervical cancer. However, with regard to the ontogenetically-defined compartments of tumor development (Müllerian) and lymph drainage (Müllerian and mesonephric), compartments at risk may also be defined consistently in endometrial cancer. This is the first report in the literature on the compartment-based surgical approach to endometrial cancer. Peritoneal mesometrial resection (PMMR) with therapeutic lymphadenectomy (tLNE) as an ontogenetic, compartment-based oncologic surgery could be beneficial for patients in terms of surgical radicalness as well as complication rates; it can be standardized for compartment-confined tumors. Supported by M Höckel, PMMR was translated to robotic surgery (rPMMR) and described step-by-step in comparison to robotic TMMR (rTMMR).
Methods: Patients (n = 42) were treated by rPMMR (n = 39) or extrafascial simple hysterectomy (n = 3) with/without bilateral pelvic and/or periaortic robotic therapeutic lymphadenectomy (rtLNE) for stage I to III endometrial cancer, according to International Federation of Gynecology and Obstetrics (FIGO) classification. Tumors were classified as intermediate/high-risk in 22 out of 40 patients (55%) and low-risk in 18 out of 40 patients (45%), and two patients showed other uterine malignancies. In 11 patients, no adjuvant external radiotherapy was performed, but chemotherapy was applied.
Results: No transition to open surgery was necessary. There were no intraoperative complications. The postoperative complication rate was 12% with venous thromboses, (n = 2), infected pelvic lymph cyst (n = 1), transient aphasia (n = 1) and transient dysfunction of micturition (n = 1). The mean difference in perioperative hemoglobin concentrations was 2.4 g/dL (± 1.2 g/dL) and one patient (2.4%) required transfusion. During follow-up (median 17 months), one patient experienced distant recurrence and one patient distant/regional recurrence of endometrial cancer (4.8%), but none developed isolated locoregional recurrence. There were two deaths from endometrial cancer during the observation period (4.8%).
Conclusions: We conclude that rPMMR and rtLNE are feasible and safe with regard to perioperative morbidity, thus, it seems promising for the treatment of intermediate/high-risk endometrial cancer in terms of surgical radicalness and complication rates. This could be particularly beneficial for morbidly obese and seriously ill patients.
Figures
References
-
- Nickles Fader A, Seamon LG, Escobar PF, Frasure HE, Havrilesky LA, Zanotti KM, Secord AA, Boggess JF, Cohn DE, Fowler JM, Skafianos G, Rossi E, Gehrig PA. Minimally invasive surgery versus laparotomy in women with high grade endometrial cancer: a multi-site study performed at high volume cancer centers. Gynecol Oncol. 2012;11:180–185. doi: 10.1016/j.ygyno.2012.04.028. - DOI - PubMed
-
- Backes FJ, Brudie LA, Farrell MR, Ahmad S, Finkler NJ, Bigsby GE, O’Malley D, Cohn DE, Holloway RW, Fowler JM. Short- and long-term morbidity and outcomes after robotic surgery for comprehensive endometrial cancer staging. Gynecol Oncol. 2012;11:546–551. doi: 10.1016/j.ygyno.2012.02.023. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
