

Sex and haemodynamics in pulmonary arterial hypertension
- PMID: 23949961
- PMCID: PMC4338984
- DOI: 10.1183/09031936.00027613
Sex and haemodynamics in pulmonary arterial hypertension
Abstract
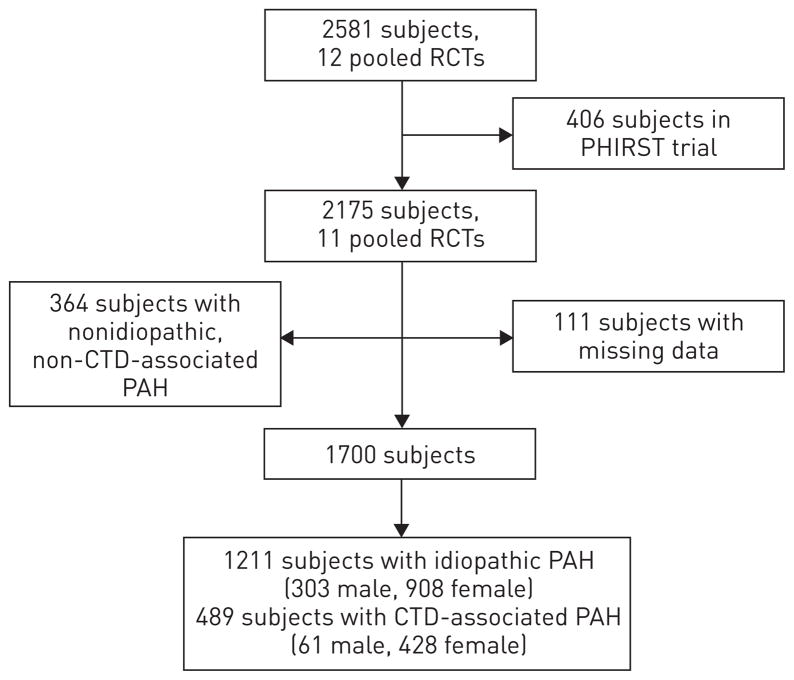
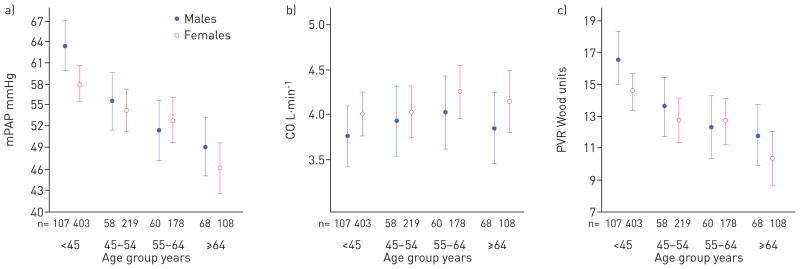
Female sex is a risk factor for pulmonary arterial hypertension (PAH), yet females have better survival than males. We sought to determine if sex was associated with baseline haemodynamics in subjects with PAH, and whether age modified these relationships. We conducted a pooled analysis from 11 randomised trials submitted to the US Food and Drug Administration. The study sample included 1211 subjects with idiopathic PAH, 25% of whom were males, and 489 subjects with connective tissue disease-associated PAH, 13% of whom were males. After multivariable adjustment, right atrial pressure was 1.36 mmHg higher (95% CI 0.44-2.27, p=0.004), cardiac index was -0.14 L · min(-1) · m(-2) lower (95% CI -0.23-0.04, p=0.01) and pulmonary vascular resistance was 1.23 Wood units higher (95% CI 0.18-2.27, p=0.02) in males compared with females. Younger males had 5.43 mmHg (95% CI 2.20-8.66, p=0.001) higher mean pulmonary arterial pressures than younger females, but these relationships were attenuated after age 45 years. In the subgroup of connective tissue disease-associated PAH, males may have had higher right atrial pressure. These findings implicate age as a modifier and provide further evidence of sexual dimorphism in PAH.
Conflict of interest statement
Conflict of interest: Disclosures can be found alongside the online version of this article at
Figures
Comment in
-
Sex matters in pulmonary arterial hypertension.Eur Respir J. 2014 Aug;44(2):553-4. doi: 10.1183/09031936.00054514. Eur Respir J. 2014. PMID: 25082914 No abstract available.
References
-
- Badesch DB, Raskob GE, Elliott CG, et al. Pulmonary arterial hypertension: baseline characteristics from the REVEAL registry. Chest. 2010;137:376–387. - PubMed
-
- Humbert M, Sitbon O, Chaouat A, et al. Pulmonary arterial hypertension in France: results from a national registry. Am J Respir Crit Care Med. 2006;173:1023–1030. - PubMed
-
- Humbert M, Sitbon O, Chaouat A, et al. Survival in patients with idiopathic, familial, and anorexigen-associated pulmonary arterial hypertension in the modern management era. Circulation. 2010;122:156–163. - PubMed
-
- Benza RL, Miller DP, Gomberg-Maitland M, et al. Predicting survival in pulmonary arterial hypertension: insights from the Registry To Evaluate Early And Long-Term Pulmonary Arterial Hypertension Disease Management (REVEAL) Circulation. 2010;122:164–172. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous