

Comparison of insulin degludec with insulin glargine in insulin-naive subjects with Type 2 diabetes: a 2-year randomized, treat-to-target trial
- PMID: 23952326
- PMCID: PMC4208679
- DOI: 10.1111/dme.12303
Comparison of insulin degludec with insulin glargine in insulin-naive subjects with Type 2 diabetes: a 2-year randomized, treat-to-target trial
Abstract
Aims: The aim of this study was to compare long-term safety and efficacy of the basal insulin analogue degludec with glargine in insulin-naive subjects with Type 2 diabetes.
Methods: This open-label trial included a 52-week core period followed by a 52-week extension. Participants were randomized 3:1 to once-daily degludec or glargine, administered with metformin ± dipeptidyl peptidase-4 inhibitors. Basal insulin was titrated to target pre-breakfast plasma glucose 3.9-4.9 mmol/l.
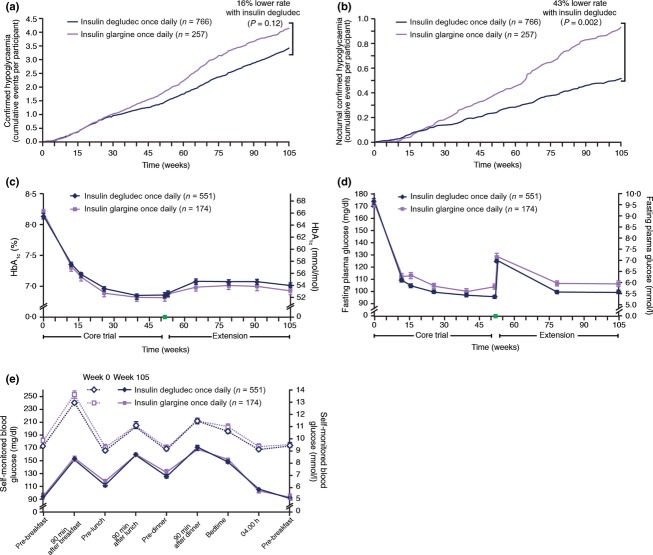
Results: At end of treatment (104 weeks), mean HbA1c reductions were similar for degludec and glargine; estimated treatment difference between degludec and glargine was 1 mmol/mol (95% CI -1 to 3) [0.07% (95% CI -0.07 to 0.22)], P = 0.339 in the extension trial set (degludec 551, glargine 174), comprising subjects who completed core trial and continued into the extension trial. Overall confirmed hypoglycaemia rates (1.72 vs. 2.05 episodes/patient-year), rates of adverse events possibly or probably related to trial product (0.19 events/patient-year), weight gain (2.7 vs. 2.4 kg) and mean daily insulin doses (0.63 U/kg) were similar between treatments in the safety analysis set (degludec 766, glargine 257) comprising all treated subjects. Rates of nocturnal confirmed hypoglycaemia (0.27 vs. 0.46 episodes/patient-year; P = 0.002) and severe hypoglycaemia (0.006 vs. 0.021 episodes/patient-year, P = 0.023) were significantly lower with degludec for the safety analysis set (analysis based on intention-to-treat full analysis set comprising all randomized subjects).
Conclusions: In Type 2 diabetes, insulin degludec in combination with oral anti-diabetic drugs, safely and effectively improves long-term glycaemic control, with a significantly lower risk of nocturnal hypoglycaemia as compared with glargine.
Trial registration: ClinicalTrials.gov NCT01193309.
© 2013 The Authors. Diabetic Medicine published by John Wiley & Sons Ltd on behalf of Diabetes UK.
Figures
Comment in
-
Insulin degludec: a new insulin for today?Diabet Med. 2013 Nov;30(11):1267. doi: 10.1111/dme.12319. Diabet Med. 2013. PMID: 24134602 No abstract available.
References
-
- Declaration of Helsinki. Ethical principles for medical research involving human subjects. J Indian Med Assoc. 2009;107:403–405. - PubMed
-
- ICH Harmonised Tripartite Guideline. Guideline for good clinical practice. J Postgrad Med. 2001;47:199–203. - PubMed
-
- Heise T, Nosek L, Bottcher SG, Hastrup H, Haahr H. Ultra-long-acting insulin degludec has a flat and stable glucose-lowering effect in type 2 diabetes. Diabetes Obes Metab. 2012;14:944–950. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
