

Endocrine and hypertensive disorders of potassium regulation: primary aldosteronism
- PMID: 23953804
- PMCID: PMC3748390
- DOI: 10.1016/j.semnephrol.2013.04.007
Endocrine and hypertensive disorders of potassium regulation: primary aldosteronism
Abstract
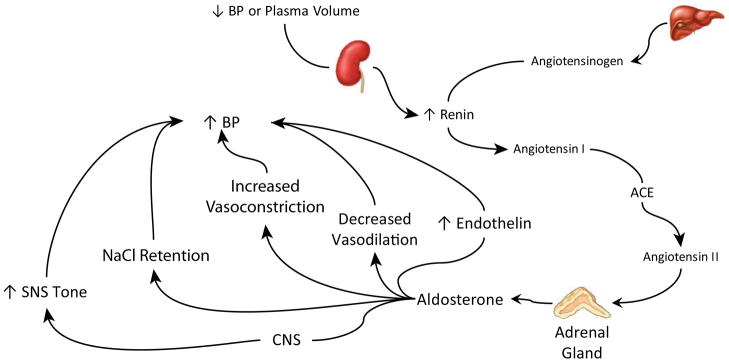
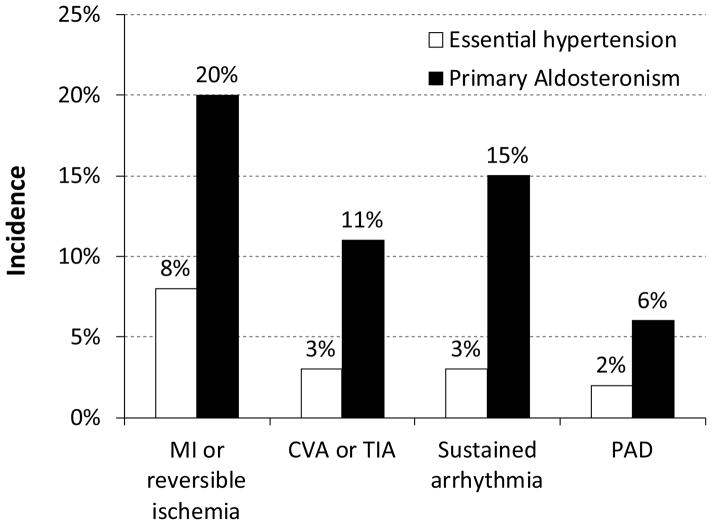
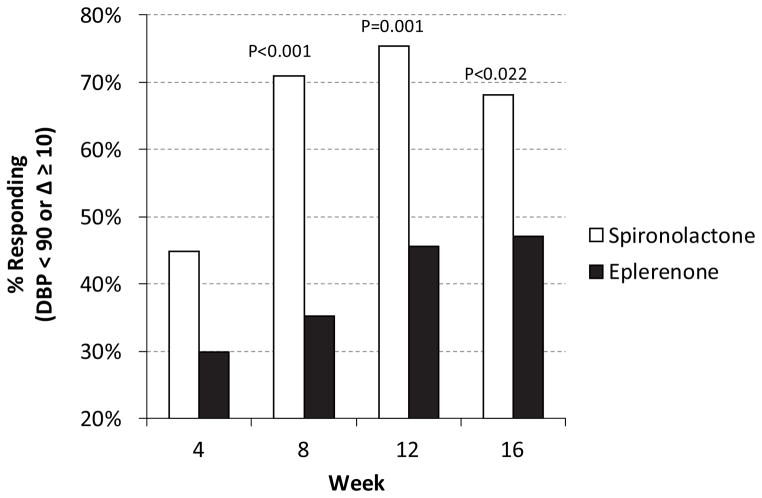
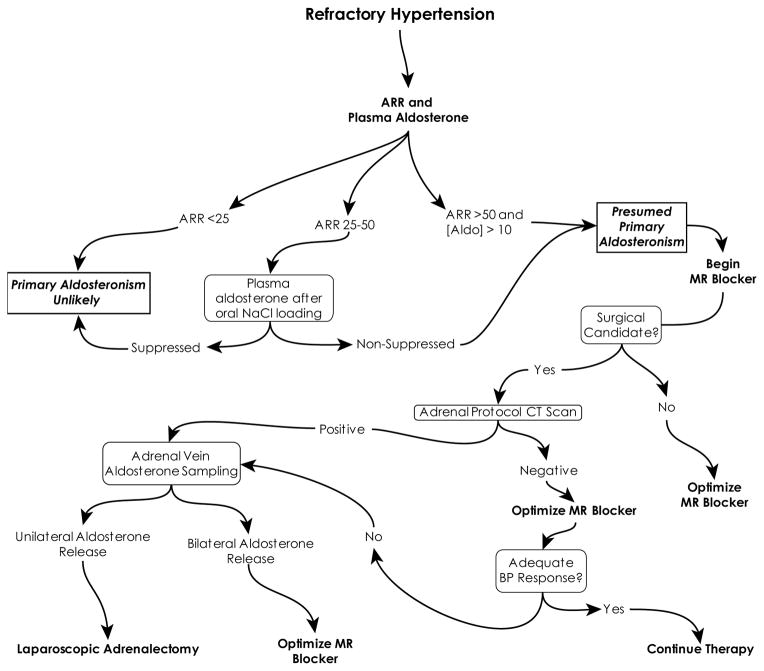
The identification of primary aldosteronism as a common cause of resistant hypertension is a significant advance in our ability to care for patients with hypertension. Primary aldosteronism is common, and when unrecognized is associated with an increased incidence of adverse cardiovascular outcomes. Identification of primary aldosteronism is based on use of the plasma aldosterone level, plasma renin activity, and the aldosterone:renin ratio. Differentiation between unilateral and bilateral autonomous adrenal aldosterone production then guides further therapy, with use of mineralocorticoid-receptor blockers for patients with bilateral autonomous adrenal aldosterone production and laparoscopic adrenalectomy for patients with unilateral autonomous aldosterone production. In this review, we discuss in detail the pathogenesis of primary aldosteronism-induced hypertension and potassium disorders, the evaluation of the patient with suspected primary aldosteronism, and the management of primary aldosteronism, both through medications and surgery.
Keywords: Aldosterone; aldosterone-producing adenoma; bilateral adrenal hyperplasia; hypertension; hypokalemia; renin.
Published by Elsevier Inc.
Figures
Similar articles
-
[Diagnosis and treatment outcome in primary aldosteronism based on a retrospective analysis of 187 cases].Orv Hetil. 2006 Jan 15;147(2):51-9. Orv Hetil. 2006. PMID: 16509213 Hungarian.
-
Diagnosing and Managing Primary Aldosteronism in Hypertensive Patients: a Case-Based Approach.Curr Cardiol Rep. 2016 Oct;18(10):97. doi: 10.1007/s11886-016-0774-1. Curr Cardiol Rep. 2016. PMID: 27566330 Review.
-
Primary aldosteronism: renaissance of a syndrome.Clin Endocrinol (Oxf). 2007 May;66(5):607-18. doi: 10.1111/j.1365-2265.2007.02775.x. Clin Endocrinol (Oxf). 2007. PMID: 17492946 Review.
-
High rate of detection of primary aldosteronism, including surgically treatable forms, after 'non-selective' screening of hypertensive patients.J Hypertens. 2003 Nov;21(11):2149-57. doi: 10.1097/00004872-200311000-00025. J Hypertens. 2003. PMID: 14597859
-
[Primary aldosteronism].Rev Prat. 2015 Jun;65(6):817-21. Rev Prat. 2015. PMID: 26298907 French.
Cited by
-
ITRAQ-based proteomic analysis reveals possible target-related proteins in human adrenocortical adenomas.BMC Genomics. 2019 Aug 16;20(1):655. doi: 10.1186/s12864-019-6030-5. BMC Genomics. 2019. PMID: 31419939 Free PMC article.
-
[Etiology of endocrine arterial hypertensions: about a series of cases].Pan Afr Med J. 2016 Apr 7;23:170. doi: 10.11604/pamj.2016.23.170.8968. eCollection 2016. Pan Afr Med J. 2016. PMID: 27303586 Free PMC article. French.
-
Hyperaldosteronism from a large adrenal adenoma in a patient with bilateral adrenal nodules.Clin Case Rep. 2019 Dec 4;8(1):55-60. doi: 10.1002/ccr3.2560. eCollection 2020 Jan. Clin Case Rep. 2019. PMID: 31998486 Free PMC article.
-
HIF1α is a direct regulator of steroidogenesis in the adrenal gland.Cell Mol Life Sci. 2021 Apr;78(7):3577-3590. doi: 10.1007/s00018-020-03750-1. Epub 2021 Jan 19. Cell Mol Life Sci. 2021. PMID: 33464382 Free PMC article.
-
Biochemical and clinical characteristics of patients with primary aldosteronism: Single centre experience.J Med Biochem. 2020 Jan 23;39(2):240-248. doi: 10.2478/jomb-2019-0035. J Med Biochem. 2020. PMID: 33033458 Free PMC article.
References
-
- Lim PO, Rodgers P, Cardale K, Watson AD, Macdonald TM. Potentially high prevalence of primary aldosteronism in a primary-care population. Lancet. 1999;353:40. - PubMed
-
- Rossi GP, Bernini G, Caliumi C, Desideri G, Fabris B, Ferri C, et al. A Prospective Study of the Prevalence of Primary Aldosteronism in 1,125 Hypertensive Patients. Journal of the American College of Cardiology. 2006;48:2293–2300. - PubMed
-
- Mosso L, Carvajal C, Gonzalez A, Barraza A, Avila F, Montero J, et al. Primary Aldosteronism and Hypertensive Disease. Hypert. 2003;42:161–165. - PubMed
-
- Gallay BJ, Ahmad S, Xu L, Toivola B, Davidson RC. Screening for primary aldosteronism without discontinuing hypertensive medications: plasma aldosterone-renin ratio. Am J Kidney Dis. 2001;37:699–705. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
