

Liver stiffness is associated with risk of decompensation, liver cancer, and death in patients with chronic liver diseases: a systematic review and meta-analysis
- PMID: 23954643
- PMCID: PMC3900882
- DOI: 10.1016/j.cgh.2013.07.034
Liver stiffness is associated with risk of decompensation, liver cancer, and death in patients with chronic liver diseases: a systematic review and meta-analysis
Abstract
Background & aims: Liver stiffness measurement (LSM), using elastography, can independently predict outcomes of patients with chronic liver diseases (CLDs). However, there is much variation in reporting and consistency of findings. We performed a systematic review and meta-analysis to evaluate the association between LSM and outcomes of patients with CLDs.
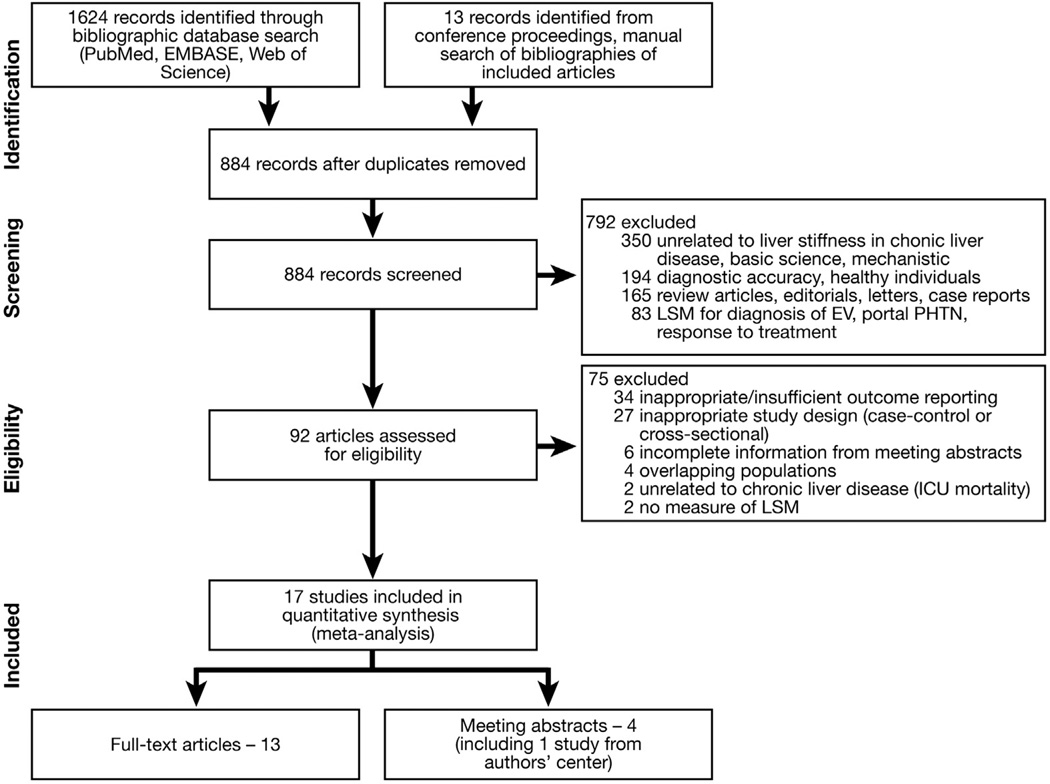
Methods: We performed a systematic review of the literature, through February 2013, for studies that followed up patients with CLDs prospectively for at least 6 months and reported the association between baseline LSM and subsequent development of decompensated cirrhosis or hepatocellular carcinoma (HCC), as well as mortality. Summary relative risk (RR) estimates per unit of LSM and 95% confidence intervals (CIs) were estimated using the random effects model.
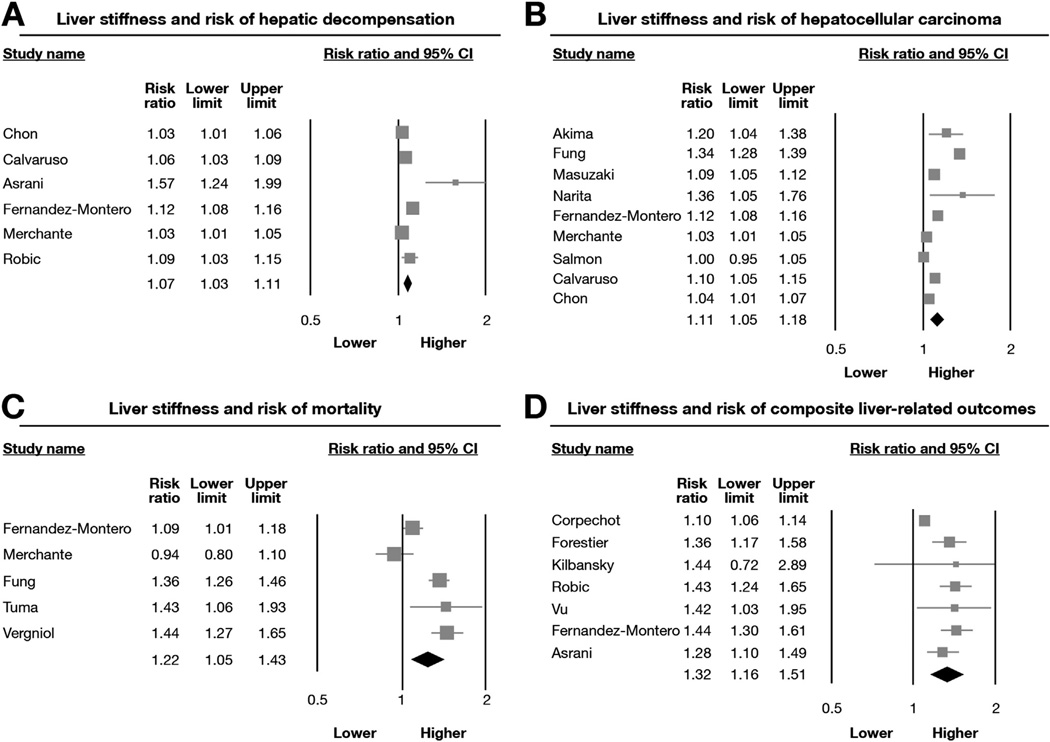
Results: Our final analysis included 17 studies, reporting on 7058 patients with CLDs. Baseline LSM was associated significantly with risk of hepatic decompensation (6 studies; RR, 1.07; 95% CI, 1.03-1.11), HCC (9 studies; RR, 1.11; 95% CI, 1.05-1.18), death (5 studies; RR, 1.22; 95% CI, 1.05-1.43), or a composite of these outcomes (7 studies; RR, 1.32; 95% CI, 1.16-1.51). We observed considerable heterogeneity among studies-primarily in the magnitude of effect, rather than the direction of effect. This heterogeneity could not be explained by variations in study locations, etiologies and stages of CLD, techniques to measure liver stiffness, adjustment for covariates, or method of imputing relationship in the meta-analysis.
Conclusions: Based on a meta-analysis of cohort studies, the degree of liver stiffness is associated with risk of decompensated cirrhosis, HCC, and death in patients with CLDs. LSM therefore might be used in risk stratification.
Keywords: CI; CLD; Cancer; Cirrhosis; Elastography; HCC; HCV; HR; HVPG; LSM; LT; MELD; MRE; Outcomes; Prognosis; RR; TE; chronic liver disease; confidence interval; hazard ratio; hepatic venous pressure gradient; hepatitis C virus; hepatocellular carcinoma; liver stiffness measurement; liver transplantation; magnetic resonance elastography; model for end-stage liver disease; relative risk; transient elastography.
Copyright © 2013 AGA Institute. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflicts of interest
This author discloses the following: Richard Ehman has intellectual property rights and a financial conflict of interest related to the technology used in this study. The remaining authors disclose no conflicts.
The Mayo Clinic also has intellectual property rights and a financial conflict of interest related to the technology used in this study. This research has been conducted in compliance with oversight by the Mayo Clinic Conflict of Interest review board.
Figures
References
-
- Manos MM, Leyden WA, Murphy RC, et al. Limitations of conventionally derived chronic liver disease mortality rates: results of a comprehensive assessment. Hepatology. 2008;47:1150–1157. - PubMed
-
- Tsochatzis EA, Bosch J, Burroughs AK. New therapeutic paradigm for patients with cirrhosis. Hepatology. 2012;56:1983–1992. - PubMed
-
- Ripoll C, Groszmann R, Garcia-Tsao G, et al. Hepatic venous pressure gradient predicts clinical decompensation in patients with compensated cirrhosis. Gastroenterology. 2007;133:481–488. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
