

Pushing harder, pushing faster, minimizing interruptions… but falling short of 2010 cardiopulmonary resuscitation targets during in-hospital pediatric and adolescent resuscitation
- PMID: 23954664
- PMCID: PMC3825766
- DOI: 10.1016/j.resuscitation.2013.07.029
Pushing harder, pushing faster, minimizing interruptions… but falling short of 2010 cardiopulmonary resuscitation targets during in-hospital pediatric and adolescent resuscitation
Abstract
Aim: The objective of this study was to evaluate the effect of instituting the 2010 Basic Life Support Guidelines on in-hospital pediatric and adolescent cardiopulmonary resuscitation (CPR) quality. We hypothesized that quality would improve, but that targets for chest compression (CC) depth would be difficult to achieve.
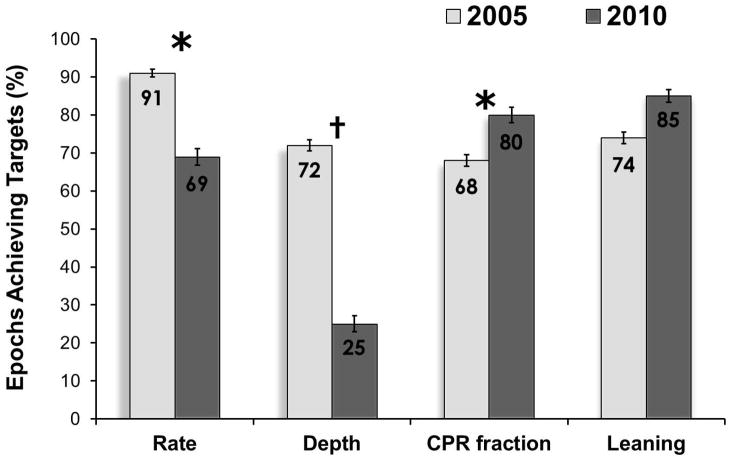
Methods: Prospective in-hospital observational study comparing CPR quality 24 months before and after release of the 2010 Guidelines. CPR recording/feedback-enabled defibrillators collected CPR data (rate (CC/min), depth (mm), CC fraction (CCF, %), leaning (%>2.5kg)). Audiovisual feedback for depth was: 2005, ≥38mm; 2010, ≥50mm; for rate: 2005, ≥90 and ≤120CC/min; 2010, ≥100 and ≤120CC/min. The primary outcome was average event depth compared with Student's t-test.
Results: 45 CPR events (25 before; 20 after) occurred, resulting in 1336 thirty-second epochs (909 before; 427 after). Compared to 2005, average event depth (50±13mm vs. 43±9mm; p=0.047), rate (113±11CC/min vs. 104±8CC/min; p<0.01), and CCF (0.94 [0.93, 0.96] vs. 0.9 [0.85, 0.94]; p=0.013) increased during 2010. CPR epochs during the 2010 period more likely to meet Guidelines for CCF (OR 1.7; CI95: 1.2-2.4; p<0.01), but less likely for rate (OR 0.23; CI95: 0.12-0.44; p<0.01), and depth (OR 0.31; CI95: 0.12-0.86; p=0.024).
Conclusions: Institution of the 2010 Guidelines was associated with increased CC depth, rate, and CC fraction; yet, achieving 2010 targets for rate and depth was difficult.
Keywords: AHA; American Heart Association; CC35; CPR; Cardiopulmonary resuscitation; Pediatric; Quality appraisal; cardiopulmonary resuscitation; chest compression.
Copyright © 2013 Elsevier Ireland Ltd. All rights reserved.
Conflict of interest statement
Figures
References
-
- Parra DA, Totapally BR, Zahn E, et al. Outcome of cardiopulmonary resuscitation in a pediatric cardiac intensive care unit. Crit Care Med. 2000;28(9):3296–3300. - PubMed
-
- Slonim AD, Patel KM, Ruttimann UE, Pollack MM. Cardiopulmonary resuscitation in pediatric intensive care units. Crit Care Med. 1997;25(12):1951–1955. - PubMed
-
- Nadkarni VM, Larkin GL, Peberdy MA, et al. First documented rhythm and clinical outcome from in-hospital cardiac arrest among children and adults. JAMA. 2006;295(1):50–57. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
