

Quantification of lower leg arterial calcifications by high-resolution peripheral quantitative computed tomography
- PMID: 23954758
- PMCID: PMC4042679
- DOI: 10.1016/j.bone.2013.08.006
Quantification of lower leg arterial calcifications by high-resolution peripheral quantitative computed tomography
Abstract
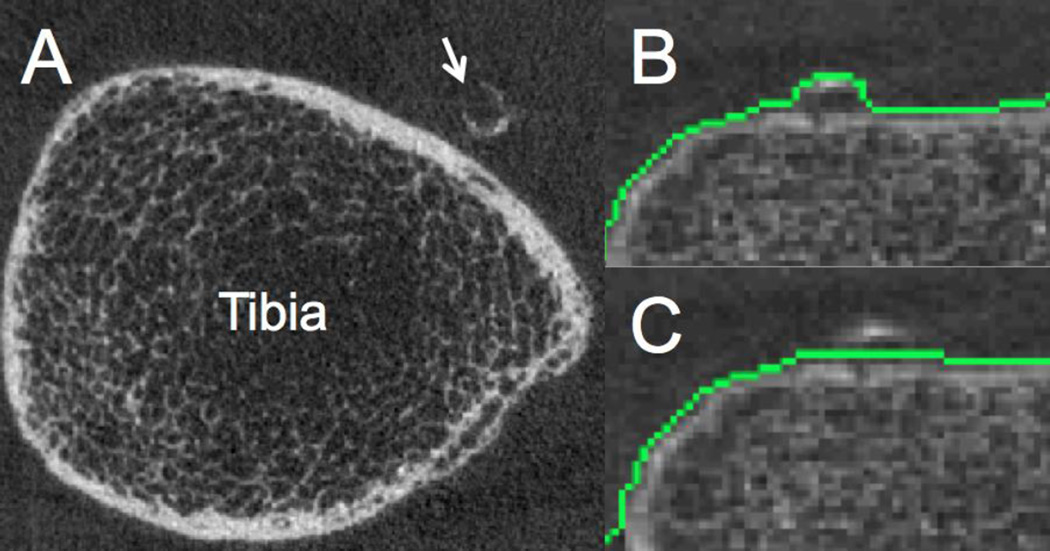
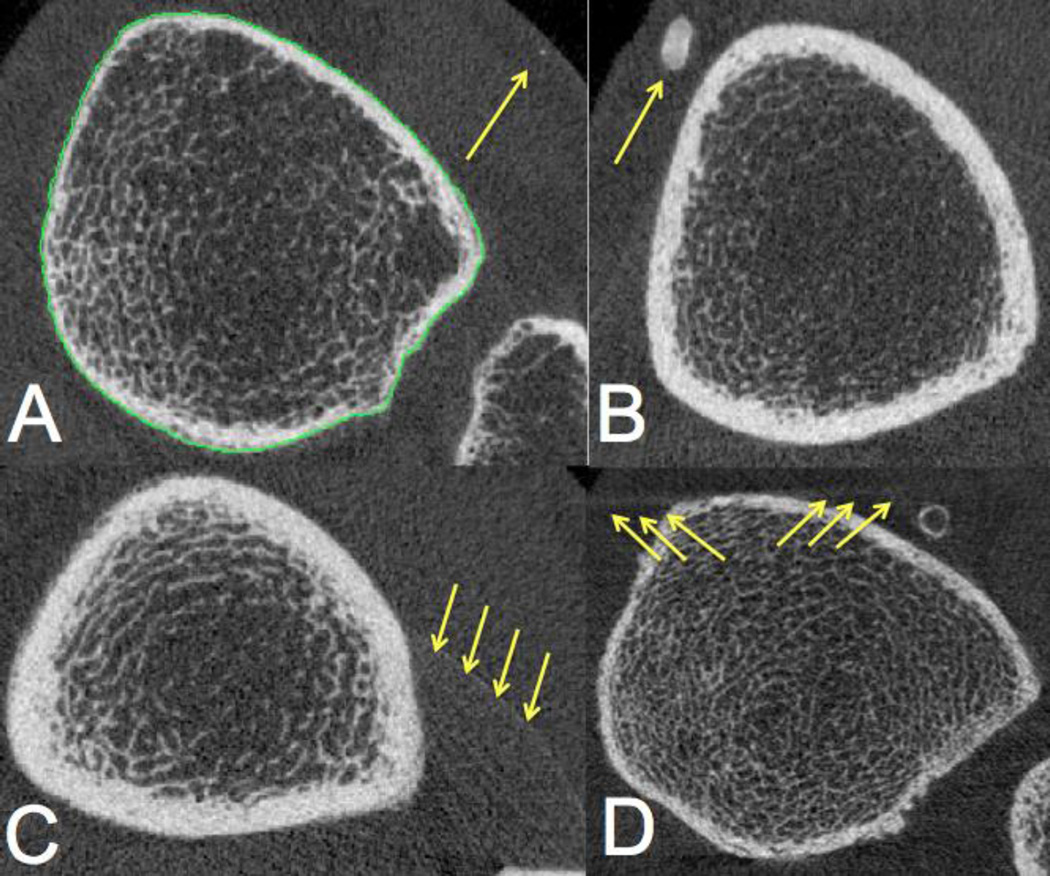
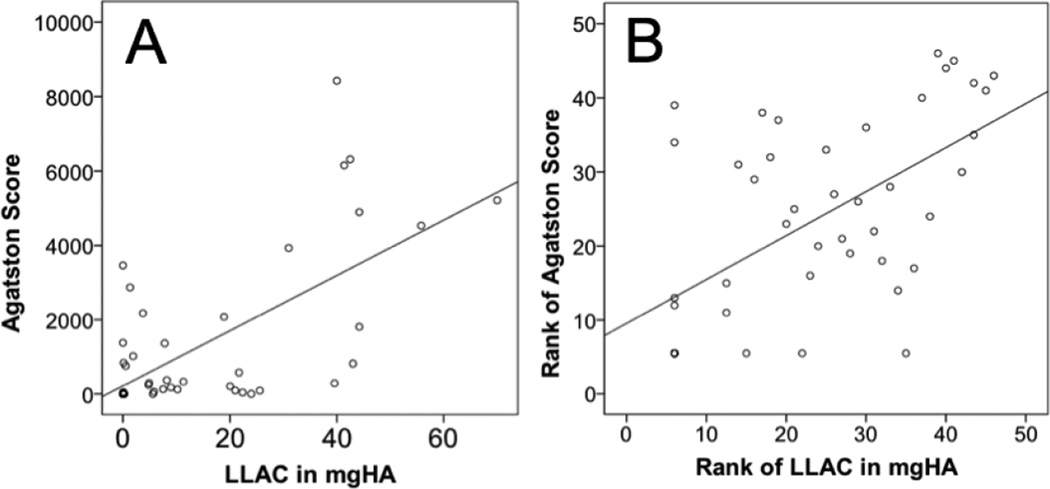
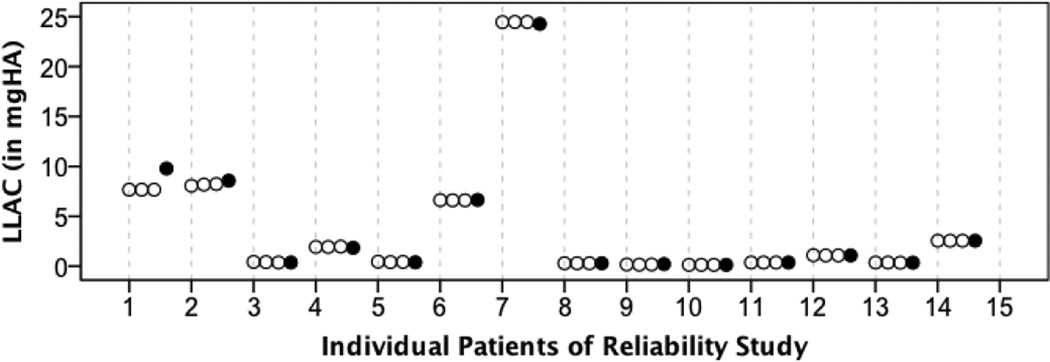
Vascular calcifications and bone health seem to be etiologically linked via common risk factors such as aging and subclinical chronic inflammation. Epidemiologic studies have shown significant associations between low bone mineral density (BMD), fragility fractures and calcifications of the coronary arteries and the abdominal aorta. In the last decade, high-resolution peripheral quantitative computed tomography (HR-pQCT) has emerged as in-vivo research tool for the assessment of peripheral bone geometry, density, and microarchitecture. Although vascular calcifications are frequently observed as incidental findings in HR-pQCT scans, they have not yet been incorporated into quantitative HR-pQCT analyses. We developed a semi-automated algorithm to quantify lower leg arterial calcifications (LLACs), captured by HR-pQCT. The objective of our study was to determine validity and reliability of the LLAC measure. HR-pQCT scans were downscaled to a voxel size of 250μm. After subtraction of bone volumes from the scans, LLACs were detected and contoured by a semi-automated, dual-threshold seed-point segmentation. LLAC mass (in mg hydroxyapatite; HA) was calculated as the product of voxel-based calcification volume (mm(3)) and mean calcification density (mgHA/cm(3))/1000. To determine validity, we compared LLACs to coronary artery calcifications (CACs), as quantified by multi-detector computed tomography (MDCT) and Agatston scoring in forty-six patients on chronic hemodialysis. Moreover, we investigated associations of LLACs with age, time on dialysis, type-2 diabetes mellitus, history of stroke, and myocardial infarction. In a second step, we determined intra- and inter-reader reliability of the LLAC measure. In the validity study, LLACs were present (>0mgHA) in 76% of patients, 78% of patients had CACs (>0mgHA). Median LLAC was 6.65 (0.08-24.40)mgHA and median CAC as expressed by Agatston score was 266.3 (15.88-1877.28). We found a significant positive correlation between LLAC and CAC (rho=0.6; p<0.01). Dialysis patients with type-2 diabetes mellitus (DM; 35%) and history of stroke (13%) had higher median LLAC than patients without those conditions (DM 20.0 fold greater, p=0.006; Stroke 5.1 fold greater, p=0.047). LLAC was positively correlated with time on dialysis (rho=0.337, p=0.029), there was a trend towards a positive association of LLAC and age (rho=0.289, p=0.053). The reliability study yielded excellent intra- and inter-reader agreement of the LLAC measure (intra-reader ICC=0.999, 95% CI=0.998-1.000; inter-reader ICC=0.998, 95% CI=0.994-0.999). Our study indicates that the LLAC measure has good validity and excellent reliability. The use of HR-pQCT for the simultaneous evaluation of arterial calcifications, peripheral bone geometry, bone density, and bone microarchitecture should facilitate future research on osteo-vascular interactions and potential associations with cardiovascular events.
Keywords: Agatston-score; HR-pQCT; Lower leg arterial calcifications; Quantification.
© 2013. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
Similar articles
-
Sex-Specific Association Patterns of Bone Microstructure and Lower Leg Arterial Calcification.Calcif Tissue Int. 2024 Nov;115(5):636-647. doi: 10.1007/s00223-024-01299-w. Epub 2024 Oct 14. Calcif Tissue Int. 2024. PMID: 39397150 Free PMC article.
-
Lower leg arterial calcification assessed by high-resolution peripheral quantitative computed tomography is associated with bone microstructure abnormalities in women.Osteoporos Int. 2016 Nov;27(11):3279-3287. doi: 10.1007/s00198-016-3660-1. Epub 2016 Jun 21. Osteoporos Int. 2016. PMID: 27325126 Free PMC article.
-
Vascular calcification relationship to vascular biomarkers and bone metabolism in advanced chronic kidney disease.Bone. 2021 Feb;143:115699. doi: 10.1016/j.bone.2020.115699. Epub 2020 Oct 20. Bone. 2021. PMID: 33091638
-
Intracranial Arterial Calcification: Prevalence, Risk Factors, and Consequences: JACC Review Topic of the Week.J Am Coll Cardiol. 2020 Sep 29;76(13):1595-1604. doi: 10.1016/j.jacc.2020.07.056. J Am Coll Cardiol. 2020. PMID: 32972537 Review.
-
Lower limb arterial calcification and its clinical relevance with peripheral arterial disease.Front Cardiovasc Med. 2023 Nov 24;10:1271100. doi: 10.3389/fcvm.2023.1271100. eCollection 2023. Front Cardiovasc Med. 2023. PMID: 38075978 Free PMC article. Review.
Cited by
-
Sex-Specific Association Patterns of Bone Microstructure and Lower Leg Arterial Calcification.Calcif Tissue Int. 2024 Nov;115(5):636-647. doi: 10.1007/s00223-024-01299-w. Epub 2024 Oct 14. Calcif Tissue Int. 2024. PMID: 39397150 Free PMC article.
-
Vascular deficits contributing to skeletal fragility in type 1 diabetes.Front Clin Diabetes Healthc. 2023 Oct 6;4:1272804. doi: 10.3389/fcdhc.2023.1272804. eCollection 2023. Front Clin Diabetes Healthc. 2023. PMID: 37867730 Free PMC article. Review.
-
CML/RAGE signal induces calcification cascade in diabetes.Diabetol Metab Syndr. 2016 Dec 28;8:83. doi: 10.1186/s13098-016-0196-7. eCollection 2016. Diabetol Metab Syndr. 2016. PMID: 28035243 Free PMC article.
-
Cellular and Molecular Mechanisms of Chronic Kidney Disease with Diabetes Mellitus and Cardiovascular Diseases as Its Comorbidities.Front Immunol. 2015 Jul 8;6:340. doi: 10.3389/fimmu.2015.00340. eCollection 2015. Front Immunol. 2015. PMID: 26217336 Free PMC article. Review.
-
The Importance of a Hierarchical Approach in Investigating the Connection Between Peripheral Artery Disease and Risk for Developing Low-Trauma Fractures: A Narrative Literature Review.J Clin Med. 2025 Feb 23;14(5):1481. doi: 10.3390/jcm14051481. J Clin Med. 2025. PMID: 40094933 Free PMC article. Review.
References
-
- Blaha M, Budoff MJ, Shaw LJ, Khosa F, Rumberger JA, Berman D, Callister T, Raggi P, Blumenthal RS, Nasir K. Absence of coronary artery calcification and all-cause mortality. JACC. Cardiovascular imaging. 2009;2:692–700. - PubMed
-
- Detrano R, Guerci AD, Carr JJ, Bild DE, Burke G, Folsom AR, Liu K, Shea S, Szklo M, Bluemke DA, O'Leary DH, Tracy R, Watson K, Wong ND, Kronmal RA. Coronary calcium as a predictor of coronary events in four racial or ethnic groups. The New England journal of medicine. 2008;358:1336–1345. - PubMed
-
- Figueiredo CP, Rajamannan NM, Lopes JB, Caparbo VF, Takayama L, Kuroishi ME, Oliveira IS, Menezes PR, Scazufca M, Bonfa E, Pereira RM. Serum phosphate and hip bone mineral density as additional factors for high vascular calcification scores in a community-dwelling: the Sao Paulo Ageing & Health Study (SPAH) Bone. 2013;52:354–359. - PubMed
-
- Schulz E, Arfai K, Liu X, Sayre J, Gilsanz V. Aortic calcification and the risk of osteoporosis and fractures. J Clin Endocrinol Metab. 2004;89:4246–4253. - PubMed
-
- Kiel DP, Kauppila LI, Cupples LA, Hannan MT, O'Donnell CJ, Wilson PW. Bone loss and the progression of abdominal aortic calcification over a 25 year period: the Framingham Heart Study. Calcified Tissue International. 2001;68:271–276. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
