

Vessel architectural imaging identifies cancer patient responders to anti-angiogenic therapy
- PMID: 23955713
- PMCID: PMC3769525
- DOI: 10.1038/nm.3289
Vessel architectural imaging identifies cancer patient responders to anti-angiogenic therapy
Abstract
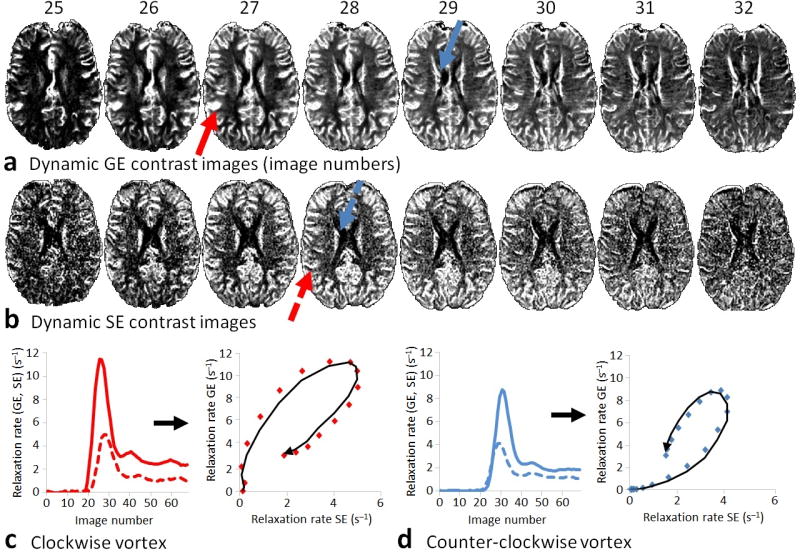
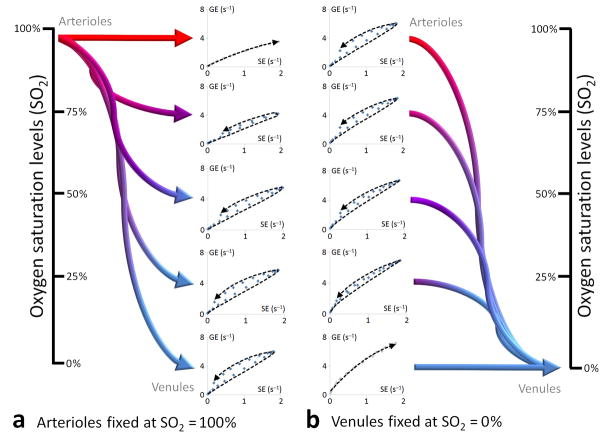
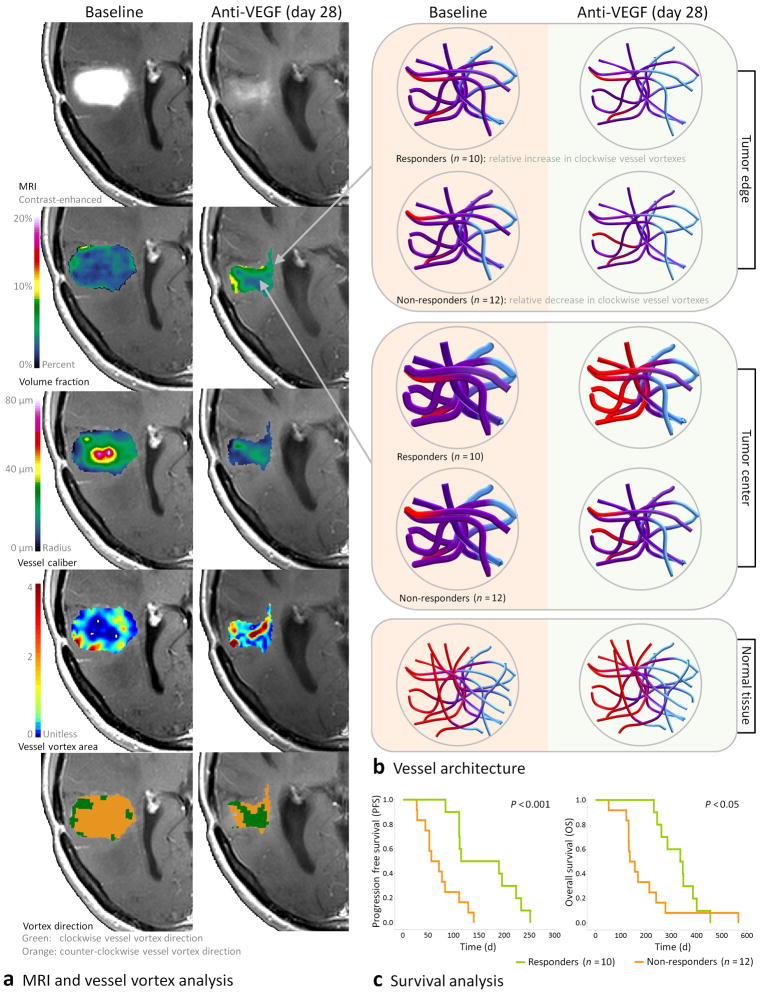
Measurement of vessel caliber by magnetic resonance imaging (MRI) is a valuable technique for in vivo monitoring of hemodynamic status and vascular development, especially in the brain. Here, we introduce a new paradigm in MRI termed vessel architectural imaging (VAI) that exploits an overlooked temporal shift in the magnetic resonance signal, forming the basis for vessel caliber estimation, and show how this phenomenon can reveal new information on vessel type and function not assessed by any other noninvasive imaging technique. We also show how this biomarker can provide new biological insights into the treatment of patients with cancer. As an example, we demonstrate using VAI that anti-angiogenic therapy can improve microcirculation and oxygen saturation and reduce vessel calibers in patients with recurrent glioblastomas and, more crucially, that patients with these responses have prolonged survival. Thus, VAI has the potential to identify patients who would benefit from therapies.
Trial registration: ClinicalTrials.gov NCT00035656.
Conflict of interest statement
Figures


References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- S10RR023043/RR/NCRR NIH HHS/United States
- S10 RR019254/RR/NCRR NIH HHS/United States
- P01CA80124/CA/NCI NIH HHS/United States
- K25 AG029415/AG/NIA NIH HHS/United States
- P01 CA080124/CA/NCI NIH HHS/United States
- R01CA129371/CA/NCI NIH HHS/United States
- UL1 RR 025758/RR/NCRR NIH HHS/United States
- S10RR019254/RR/NCRR NIH HHS/United States
- S10 RR023401/RR/NCRR NIH HHS/United States
- R01CA137254/CA/NCI NIH HHS/United States
- 5R01NS060918/NS/NINDS NIH HHS/United States
- R01 CA137254/CA/NCI NIH HHS/United States
- S10 RR021110/RR/NCRR NIH HHS/United States
- S10 RR019307/RR/NCRR NIH HHS/United States
- K25AG029415/AG/NIA NIH HHS/United States
- K24CA125440/CA/NCI NIH HHS/United States
- R21 CA117079/CA/NCI NIH HHS/United States
- R01 CA129371/CA/NCI NIH HHS/United States
- S10RR023401/RR/NCRR NIH HHS/United States
- K24 CA125440/CA/NCI NIH HHS/United States
- M01 RR001066/RR/NCRR NIH HHS/United States
- R21CA117079/CA/NCI NIH HHS/United States
- S10RR021110/RR/NCRR NIH HHS/United States
- U01 CA154601/CA/NCI NIH HHS/United States
- UL1 RR025758/RR/NCRR NIH HHS/United States
- S10RR019307/RR/NCRR NIH HHS/United States
- R01 NS060918/NS/NINDS NIH HHS/United States
- S10 RR023043/RR/NCRR NIH HHS/United States
- M01-RR-01066/RR/NCRR NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
