

The comparative evaluation of intravenous with intramuscular clonidine for suppression of hemodynamic changes in laparoscopic cholecystectomy
- PMID: 23956720
- PMCID: PMC3737696
- DOI: 10.4103/1658-354X.114070
The comparative evaluation of intravenous with intramuscular clonidine for suppression of hemodynamic changes in laparoscopic cholecystectomy
Abstract
Background: Clonidine diminishes stress response by reducing circulating catecholamines and hence increases perioperative circulatory stability in patients undergoing laparoscopic surgeries. The aim of this study was to compare intravenous (IV) clonidine (2 μg/kg) with intramuscular (IM) clonidine (2 μg/kg) for attenuation of stress response in laproscopic surgeries.
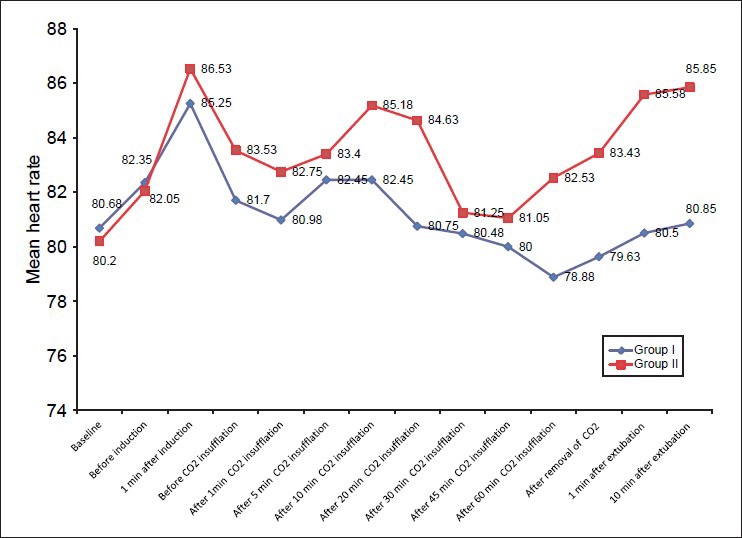
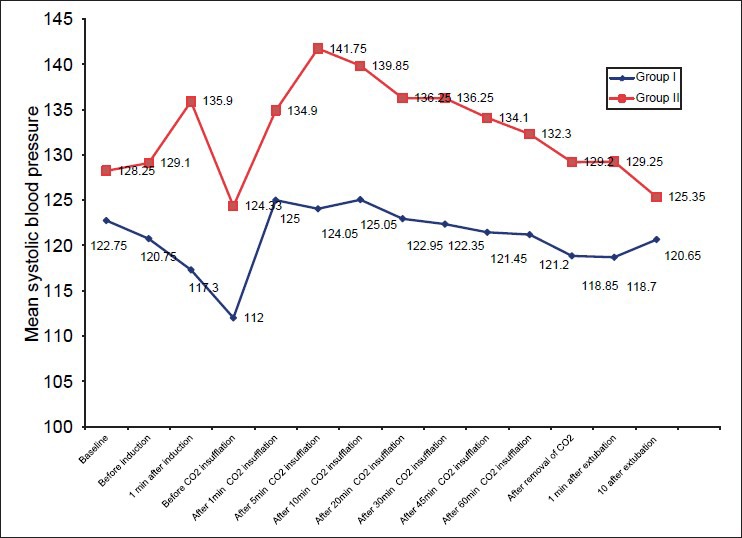
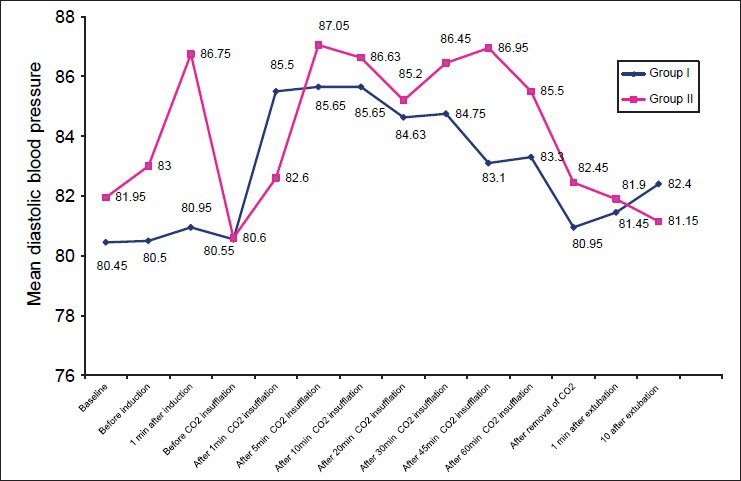
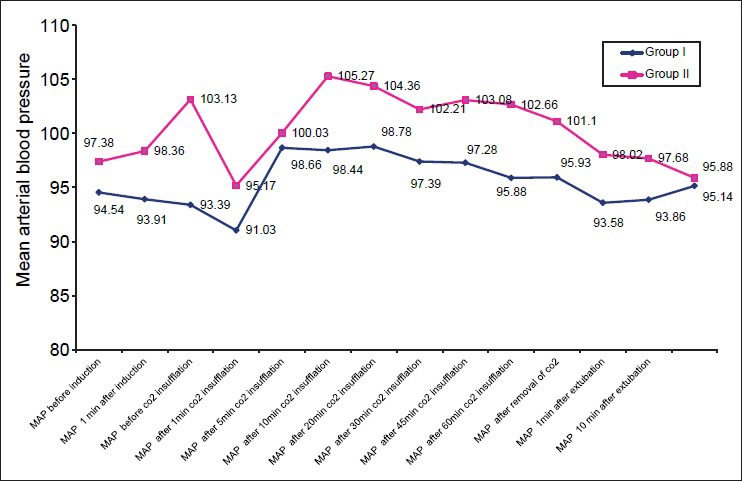
Methods: Eighty adult patients classified as ASA physical status I or II, aged between 20 and 60 years undergoing elective cholecystectomy under general anesthesia were enrolled for a prospective, randomized, and double-blind controlled trial. They received either IV clonidine (2 μg/kg) 15 min prior to the scheduled surgery (Group I) or IM clonidine (2 μg/kg) 60-90 min prior to the scheduled surgery (Group II). Hemodynamic variables (Heart rate, systolic (SBP), diastolic (DBP), mean arterial pressure (MAP)), SpO2 and EtCO2 were recorded at specific times - baseline, prior to induction, 1 min after intubation, before CO2, insufflation, after CO2 insufflation at 1,5,10,20,30,45,60 min, after release of CO2, at 1 and 10 minutes after extubation. Secondary outcomes included evaluation of adverse effect profile of the two groups.
Results: No significant difference was observed in the HR throughout the intraoperative period in between the two groups (P>0.05). There was statistically significant difference in SBP between the two groups starting from 1 minute after induction till 1 min after extubation (P<0.05) but not in DBP except at 1 minute after intubation (P=0.042). Significant difference in MAP was noted at 1 minute after intubation (P=0.004) and then from 5 minutes after CO2 insufflation to 1 minute after extubation (P<0.05). Incidence of adverse effects were higher in group II (P=0.02) especially incidence of hypertension requiring treatment (0.006).
Conclusion: We conclude that under the conditions of this study, hemodynamic parameters (SBP, DBP and MAP) were better maintained in the IV as compared to the IM route that had significantly higher incidence of hypertension requiring treatment.
Keywords: Clonidine; hemodynamic response; laproscopic cholecystectomy; pneumoperitoneum; stress response.
Conflict of interest statement
Figures
References
-
- Matovic E, Hasukic S, Ljuca F, Halilovic H. Quality of life in patients after laparoscopic and open cholecystectomy. Med Arch. 2012;66:97–100. - PubMed
-
- Leonard IE, Cunningham AJ. Anaesthetic considerations for laparoscopic cholecystectomy. Best Pract Res Clin Anaesthesiol. 2002;16:1–20. - PubMed
-
- Joris JL, Chiche JD, Canivet JL, Jacquet NJ, Legros JJ, Lamy ML. Hemodynamic changes induced by laparoscopy and their endocrine correlates: Effects of clonidine. J Am Coll Cardiol. 1998;32:1389–96. - PubMed
-
- Koivusalo AM, Scheinin M, Tikkanen I, Yli-Suomu T, Ristkari S, Laakso J, et al. Effects of esmolol on haemodynamic response to CO2 pneumoperitoneum for laparoscopic surgery. Acta Anaesthesiol Scand. 1998;42:510–7. - PubMed
-
- De Oliveira GS, Jr, Fitzgerald P, Streicher LF, Marcus RJ, McCarthy RJ. Systemic lidocaine to improve postoperative quality of recovery after ambulatory laparoscopic surgery. Anesth Analg. 2012;115:262–7. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
