

Acute myocardial infarction and massive pulmonary embolus presenting as cardiac arrest: initial rhythm as a diagnostic clue
- PMID: 23956886
- PMCID: PMC3728547
- DOI: 10.1155/2013/343918
Acute myocardial infarction and massive pulmonary embolus presenting as cardiac arrest: initial rhythm as a diagnostic clue
Abstract
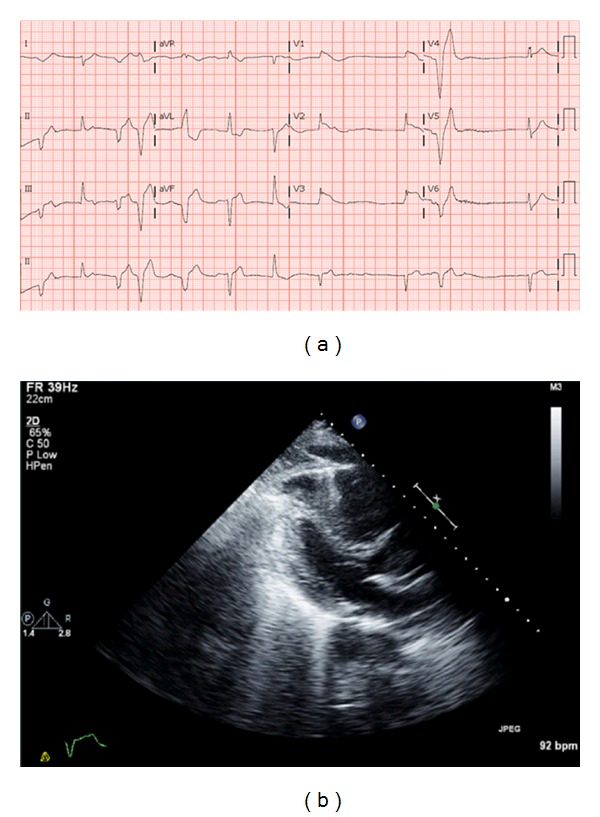
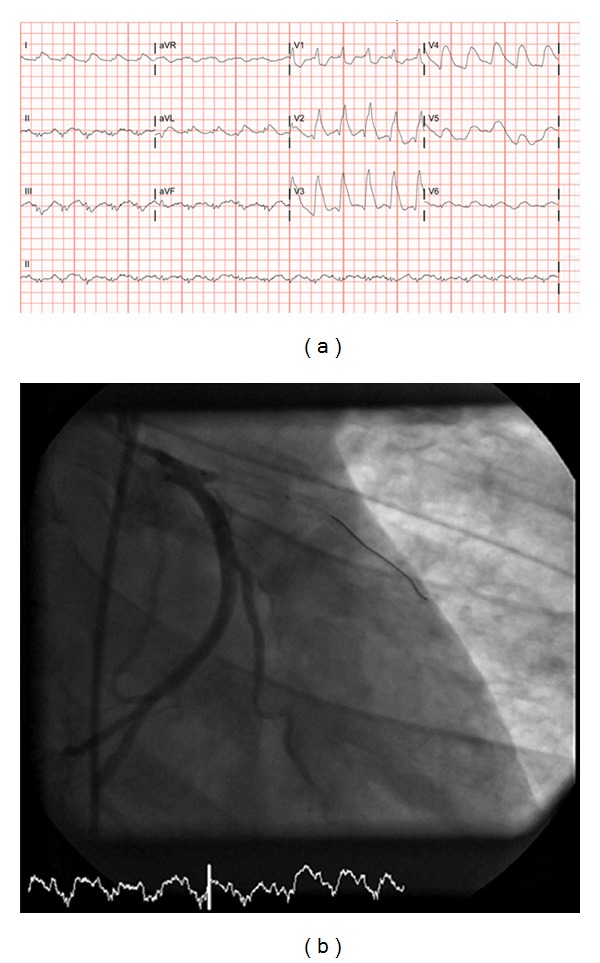
Myocardial infarction (MI) and massive pulmonary embolism (MPE) are common causes of cardiac arrest. We present two cases with similar clinical presentation and EKG findings but different initial rhythms. Case 1. A 55-year-old African American male (AAM) was brought to the emergency room (ER) with cardiac arrest and pulseless electrical activity (PEA). Twelve-lead electrocardiogram (EKG) was suggestive of ST segment elevations (STEs) in anterolateral leads. Coronary angiogram did not reveal any significant obstruction. An echocardiogram was suggestive of a pulmonary embolus (PE). Autopsy revealed a saddle PE. Case 2. A 45-year-old AAM with a history of coronary artery disease was brought to the ER after ventricular fibrillation (VF) arrest. Twelve-lead EKG was suggestive of STE in anterior leads. Coronary angiogram revealed in-stent thrombosis. In cardiac arrests, distinguishing the two major etiologies (MI and MPE) can be challenging. PEA is more commonly associated with MPE versus MI due to near complete obstruction of pulmonary blood flow with an intact electrical conduction system. MI is more commonly associated with VF as the electrical conduction system is affected more often by ischemia. In conclusion, the previous cases illustrate that initial rhythm may be a vital diagnostic clue.
Figures
Similar articles
-
Pulseless electrical activity with witnessed arrest as a predictor of sudden death from massive pulmonary embolism in outpatients.Resuscitation. 2001 Jun;49(3):265-72. doi: 10.1016/s0300-9572(00)00374-9. Resuscitation. 2001. PMID: 11719120
-
Association of initial recorded rhythm and underlying cardiac disease in sudden cardiac arrest.Resuscitation. 2018 Jan;122:76-78. doi: 10.1016/j.resuscitation.2017.11.064. Epub 2017 Nov 27. Resuscitation. 2018. PMID: 29191702
-
ST-segment elevation in V1-V4 in acute pulmonary embolism: a case presentation and review of literature.Eur Heart J Acute Cardiovasc Care. 2016 Dec;5(8):579-586. doi: 10.1177/2048872615604273. Epub 2015 Sep 15. Eur Heart J Acute Cardiovasc Care. 2016. PMID: 26373811 Review.
-
Pulseless Electrical Activity Cardiac Arrest.J Educ Teach Emerg Med. 2020 Jan 15;5(1):S1-S25. doi: 10.21980/J8Z055. eCollection 2020 Jan. J Educ Teach Emerg Med. 2020. PMID: 37465603 Free PMC article.
-
Intravascular Cooling Catheter-Related Venous Thromboembolism After Hypothermia: A Case Report and Review of the Literature.Ther Hypothermia Temp Manag. 2018 Jun;8(2):117-120. doi: 10.1089/ther.2017.0059. Epub 2018 Mar 23. Ther Hypothermia Temp Manag. 2018. PMID: 29570428 Review.
References
-
- Vanbrabant P, Dhondt E, Billen P, Sabbe M. Aetiology of unsuccessful prehospital witnessed cardiac arrest of unclear origin. European Journal of Emergency Medicine. 2006;13(3):144–147. - PubMed
-
- Raghav KP, Makkuni P, Figueredo VM. A review of electrocardiography in pulmonary embolism: recognizing pulmonary embolus masquerading as ST-elevation myocardial infarction. Reviews in Cardiovascular Medicine. 2011;12(3):157–163. - PubMed
-
- Bailen MR, Cuadra JAR, de Hoyos EA. Thrombolysis during cardiopulmonary resuscitation in fulminant pulmonary embolism: a review. Critical Care Medicine. 2001;29(11):2211–2219. - PubMed
-
- Desbiens NA. Simplifying the diagnosis and management of pulseless electrical activity in adults: a qualitative review. Critical Care Medicine. 2008;36(2):391–396. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
