

Randomized noninferiority trial of reduced high-dose volume versus standard volume radiation therapy for muscle-invasive bladder cancer: results of the BC2001 trial (CRUK/01/004)
- PMID: 23958147
- PMCID: PMC3753507
- DOI: 10.1016/j.ijrobp.2013.06.2044
Randomized noninferiority trial of reduced high-dose volume versus standard volume radiation therapy for muscle-invasive bladder cancer: results of the BC2001 trial (CRUK/01/004)
Erratum in
- Int J Radiat Oncol Biol Phys. 2013 Dec 1;87(5):860
Abstract
Purpose: To test whether reducing radiation dose to uninvolved bladder while maintaining dose to the tumor would reduce side effects without impairing local control in the treatment of muscle-invasive bladder cancer.
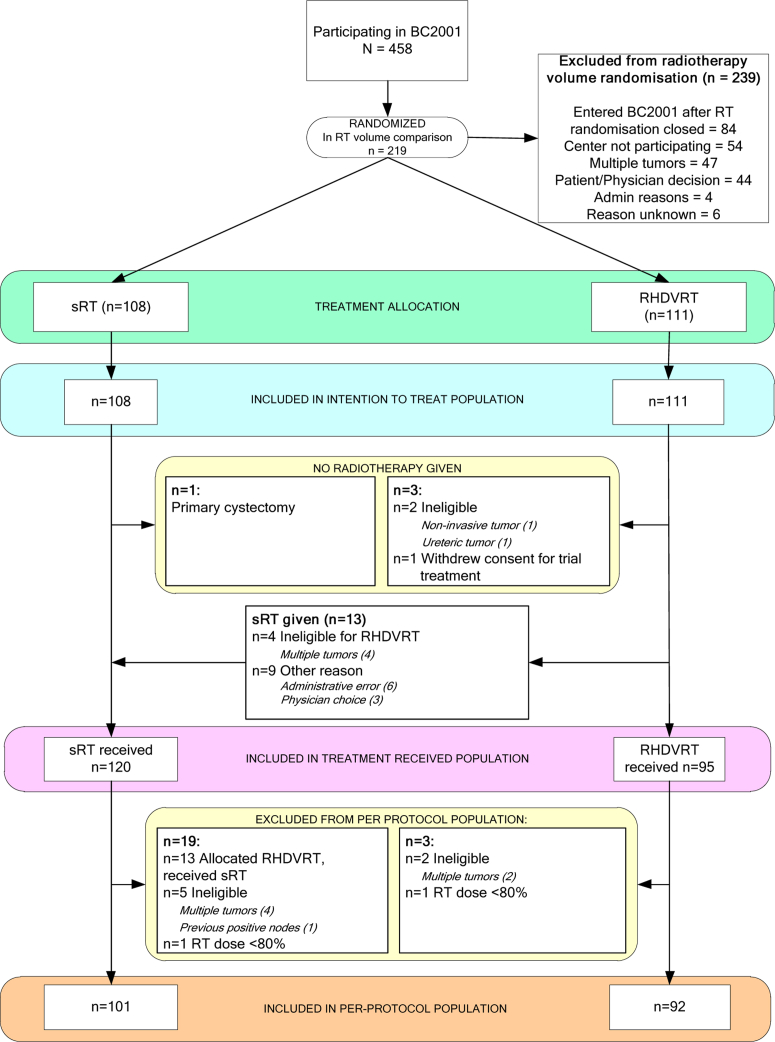
Methods and materials: In this phase III multicenter trial, 219 patients were randomized to standard whole-bladder radiation therapy (sRT) or reduced high-dose volume radiation therapy (RHDVRT) that aimed to deliver full radiation dose to the tumor and 80% of maximum dose to the uninvolved bladder. Participants were also randomly assigned to receive radiation therapy alone or radiation therapy plus chemotherapy in a partial 2 × 2 factorial design. The primary endpoints for the radiation therapy volume comparison were late toxicity and time to locoregional recurrence (with a noninferiority margin of 10% at 2 years).
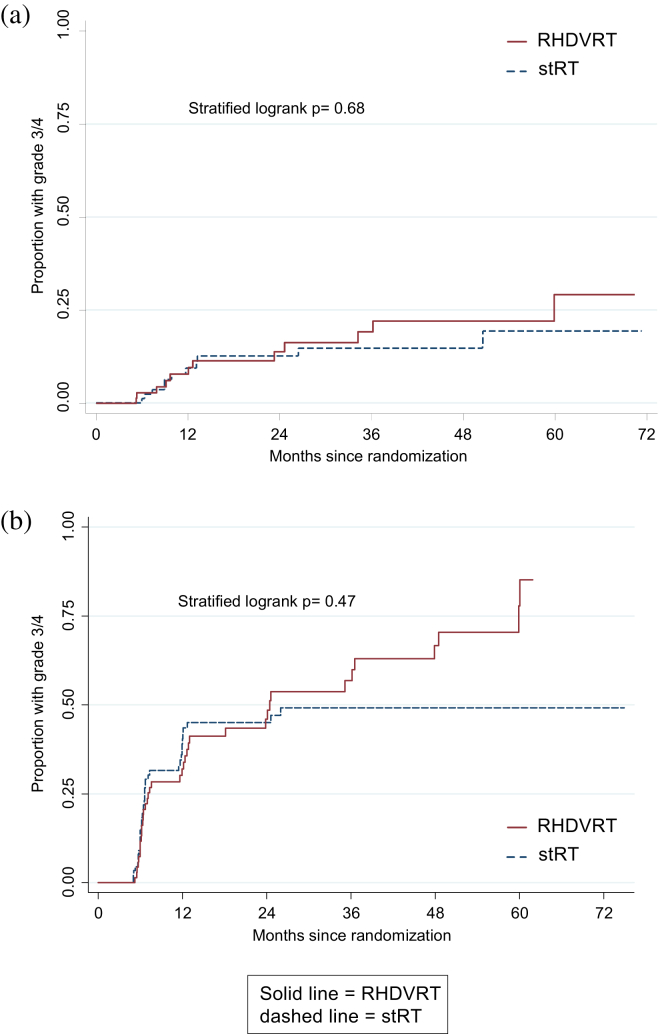
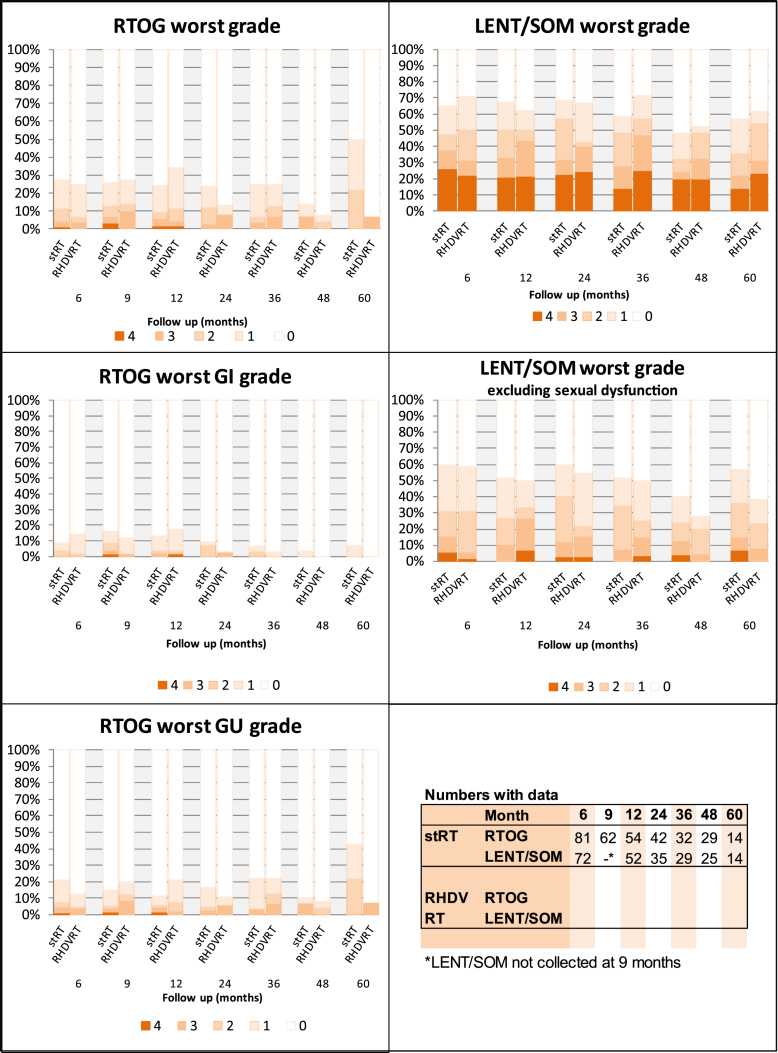
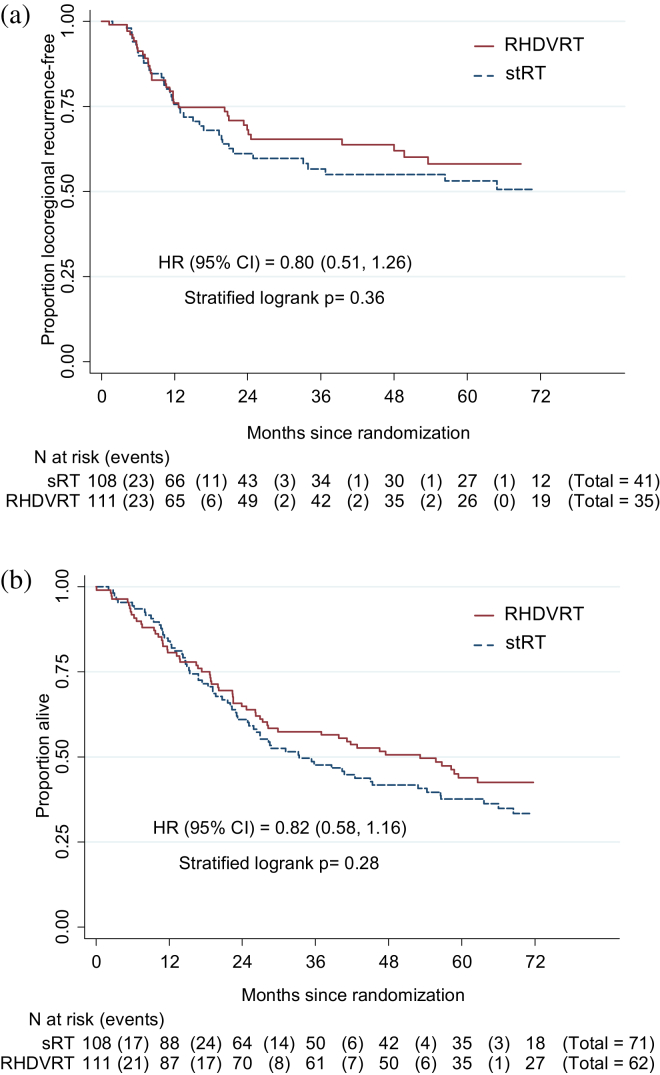
Results: Overall incidence of late toxicity was less than predicted, with a cumulative 2-year Radiation Therapy Oncology Group grade 3/4 toxicity rate of 13% (95% confidence interval 8%, 20%) and no statistically significant differences between groups. The difference in 2-year locoregional recurrence free rate (RHDVRT - sRT) was 6.4% (95% confidence interval -7.3%, 16.8%) under an intention to treat analysis and 2.6% (-12.8%, 14.6%) in the "per-protocol" population.
Conclusions: In this study RHDVRT did not result in a statistically significant reduction in late side effects compared with sRT, and noninferiority of locoregional control could not be concluded formally. However, overall low rates of clinically significant toxicity combined with low rates of invasive bladder cancer relapse confirm that (chemo)radiation therapy is a valid option for the treatment of muscle-invasive bladder cancer.
Copyright © 2013 Elsevier Inc. All rights reserved.
Figures
References
-
- International Agency for Research on Cancer. GLOBOCAN 2008. Available at: http://globocan.iarc.fr. Accessed August 24, 2010.
-
- Stein J.P., Lieskovsky G., Cote R. Radical cystectomy in the treatment of invasive bladder cancer: Long-term results in 1,054 patients. J Clin Oncology. 2001;19:666–675. - PubMed
-
- Rodel C. Combined-modality treatment and selective organ preservation in invasive bladder cancer: Long-term results. J Clin Oncology. 2002;20:3061–3071. - PubMed
-
- National Institute for Clinical Excellence . NICE; London: 2002. Guidance on Cancer Services. Improving Outcomes in Urological Cancers: The Manual.
-
- Cooke P., Dunn J., Latief T. Long-term risk of salvage cystectomy after radiotherapy for muscle-invasive bladder cancer. Eur Urol. 2000;38:279–286. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
