

Hyperoxemia and long-term outcome after traumatic brain injury
- PMID: 23958227
- PMCID: PMC4056982
- DOI: 10.1186/cc12856
Hyperoxemia and long-term outcome after traumatic brain injury
Abstract
Introduction: The relationship between hyperoxemia and outcome in patients with traumatic brain injury (TBI) is controversial. We sought to investigate the independent relationship between hyperoxemia and long-term mortality in patients with moderate-to-severe traumatic brain injury.
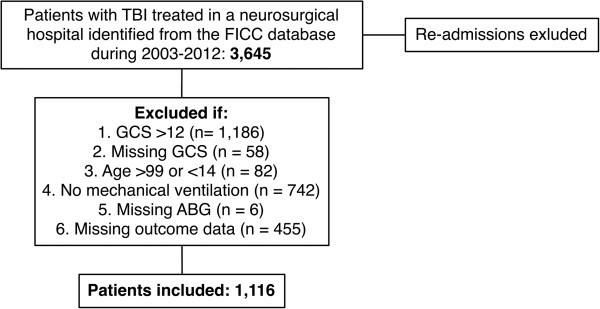
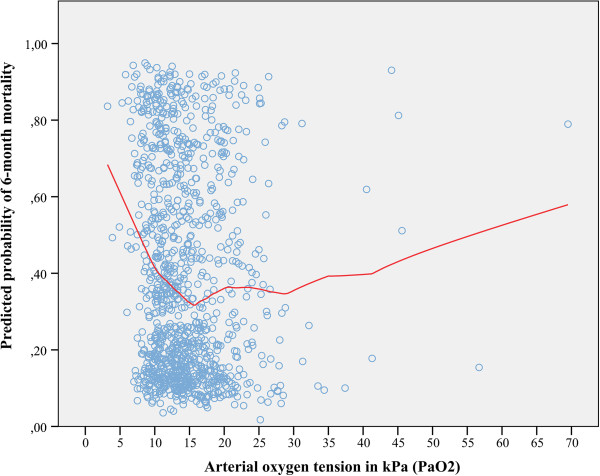
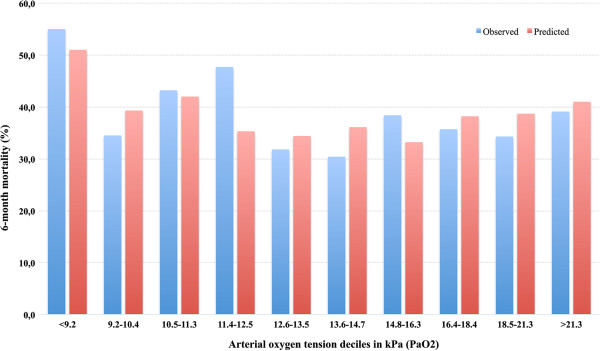
Methods: The Finnish Intensive Care Consortium database was screened for mechanically ventilated patients with a moderate-to-severe TBI. Patients were categorized, according to the highest measured alveolar-arterial O₂ gradient or the lowest measured PaO₂ value during the first 24 hours of ICU admission, to hypoxemia (<10.0 kPa), normoxemia (10.0 to 13.3 kPa) and hyperoxemia (>13.3 kPa). We adjusted for markers of illness severity to evaluate the independent relationship between hyperoxemia and 6-month mortality.
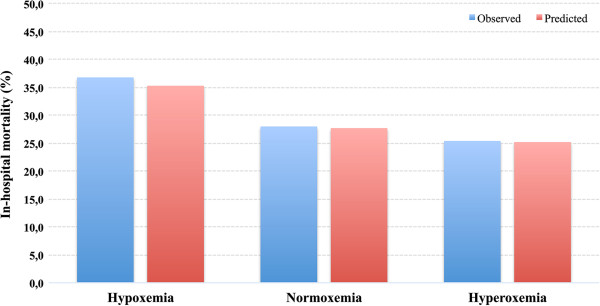
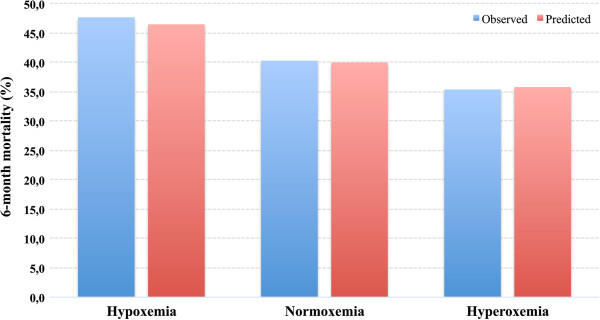
Results: A total of 1,116 patients were included in the study, of which 16% (n = 174) were hypoxemic, 51% (n = 567) normoxemic and 33% (n = 375) hyperoxemic. The total 6-month mortality was 39% (n = 435). A significant association between hyperoxemia and a decreased risk of mortality was found in univariate analysis (P = 0.012). However, after adjusting for markers of illness severity in a multivariate logistic regression model hyperoxemia showed no independent relationship with 6-month mortality (hyperoxemia vs. normoxemia OR 0.88, 95% CI 0. 63 to 1.22, P = 0.43; hyperoxemia vs. hypoxemia OR 0.97, 95% CI 0.63 to 1.50, P = 0.90).
Conclusion: Hyperoxemia in the first 24 hours of ICU admission after a moderate-to-severe TBI is not predictive of 6-month mortality.
Figures
Comment in
-
Eubaric hyperoxia: controversies in the management of acute traumatic brain injury.Crit Care. 2013 Oct 16;17(5):197. doi: 10.1186/cc13065. Crit Care. 2013. PMID: 24499710 Free PMC article.
References
-
- Maas AI, Dearden M, Teasdale GM, Braakman R, Cohadon F, Iannotti F, Karimi A, Lapierre F, Murray G, Ohman J, Persson L, Servadei F, Stocchetti N, Unterberg A. EBIC-guidelines for management of severe head injury in adults. European Brain Injury Consortium. Acta Neurochir (Wien) 1997;17:286–294. doi: 10.1007/BF01808823. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
