

Supramalleolar osteotomies for degenerative joint disease of the ankle joint: indication, technique and results
- PMID: 23959222
- PMCID: PMC3764298
- DOI: 10.1007/s00264-013-2030-2
Supramalleolar osteotomies for degenerative joint disease of the ankle joint: indication, technique and results
Abstract
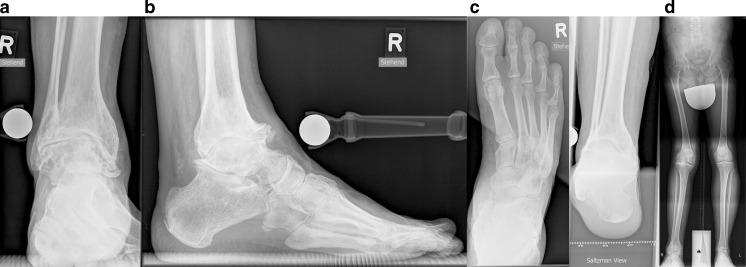
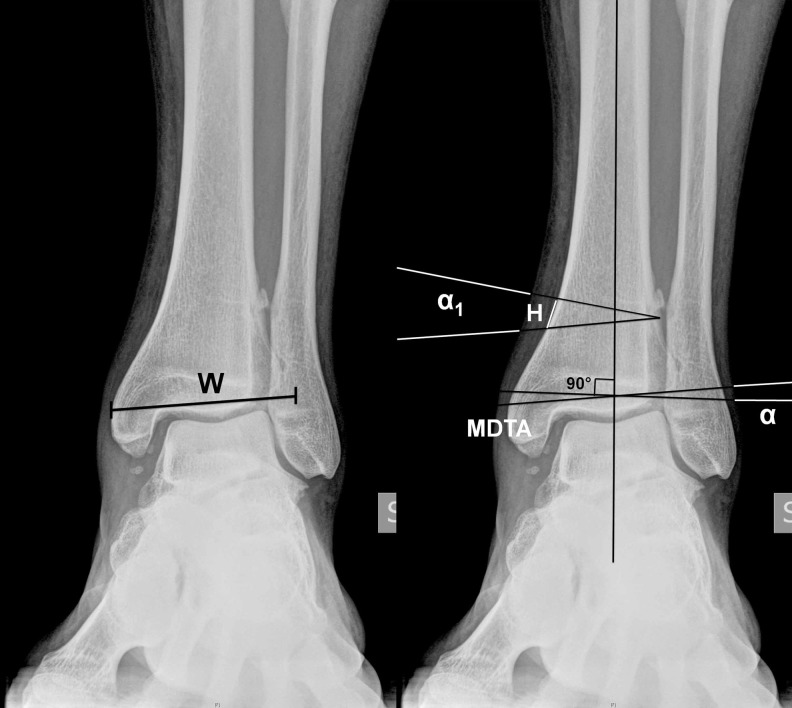
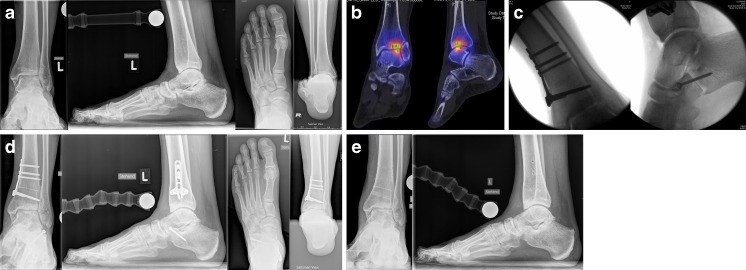
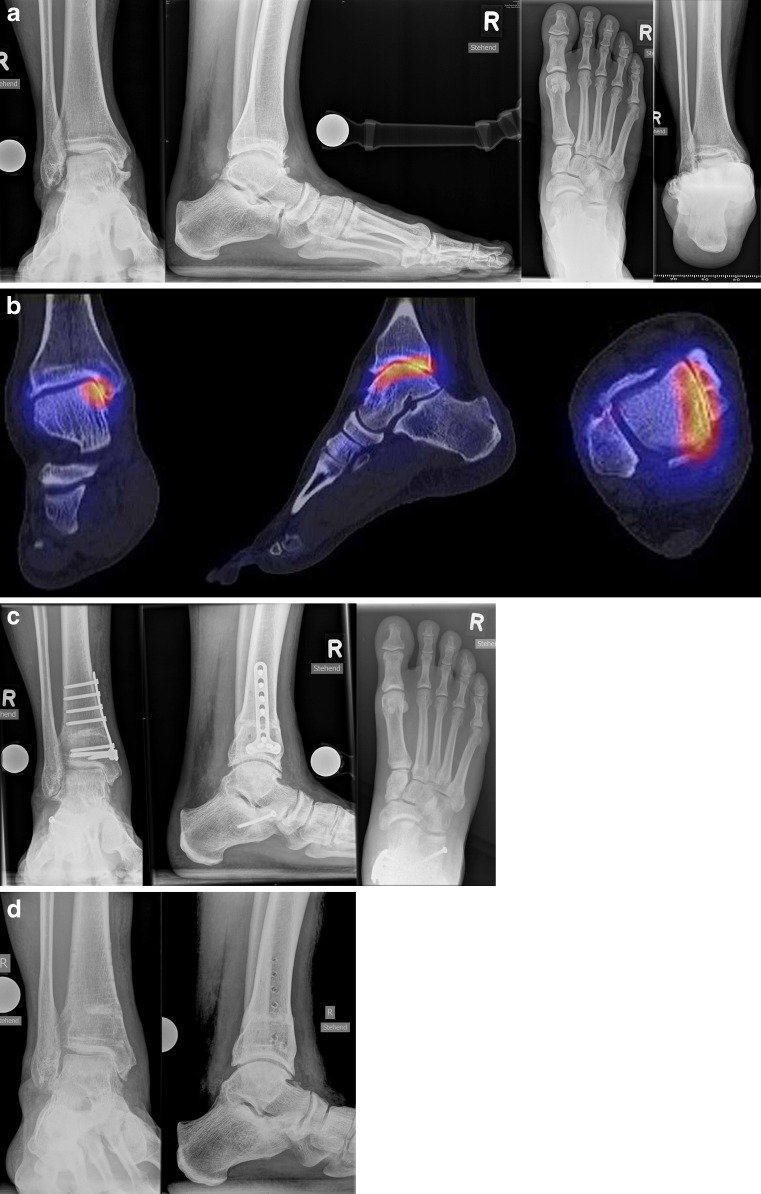
Patients with varus or valgus hindfoot deformities usually present with asymmetric ankle osteoarthritis. In-vitro biomechanical studies have shown that varus or valgus hindfoot deformity may lead to altered load distribution in the tibiotalar joint which may result in medial (varus) or lateral (valgus) tibiotalar joint degeneration in the short or medium term. The treatment of asymmetric ankle osteoarthritis remains challenging, because more than half of the tibiotalar joint surface is usually preserved. Therefore, joint-sacrificing procedures like total ankle replacement or ankle arthrodesis may not be the most appropriate treatment options. The shortand midterm results following realignment surgery, are very promising with substantial pain relief and functional improvement observed post-operatively. In this review article we describe the indications, surgical techniques, and results from of realignment surgery of the ankle joint in the current literature.
Figures


References
-
- Buckwalter JA, Saltzman C, Brown T (2004) The impact of osteoarthritis: implications for research. Clin Orthop Relat Res (427 Suppl):S6–S15 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
