

Bone strength and structural deficits in children and adolescents with a distal forearm fracture resulting from mild trauma
- PMID: 23959563
- PMCID: PMC4074503
- DOI: 10.1002/jbmr.2071
Bone strength and structural deficits in children and adolescents with a distal forearm fracture resulting from mild trauma
Abstract
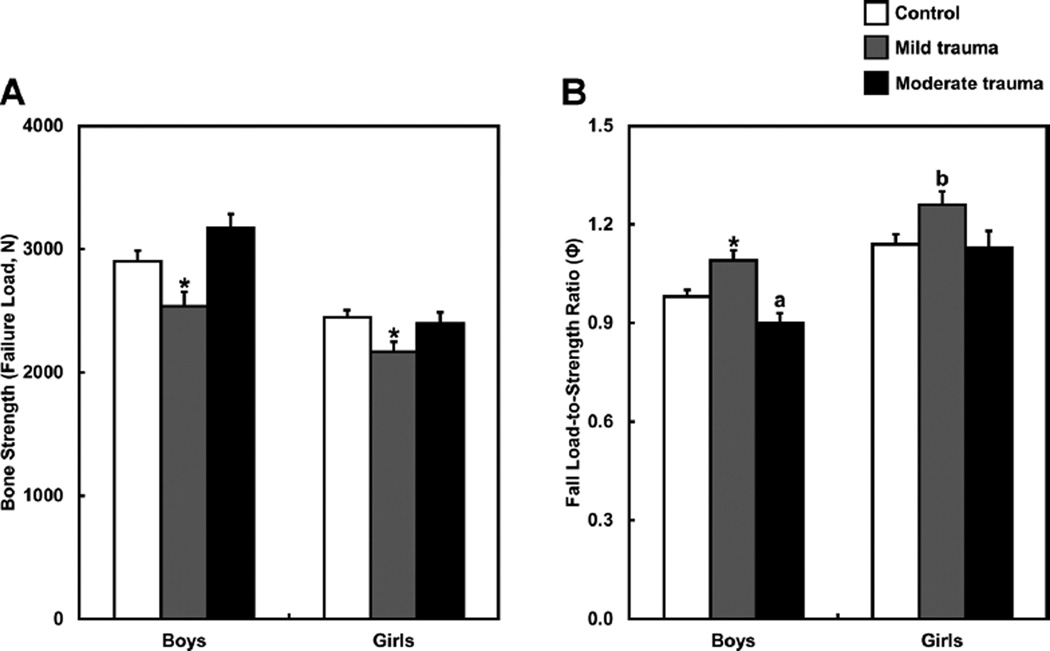
Although distal forearm fractures (DFFs) are common during childhood and adolescence, it is unclear whether they reflect underlying skeletal deficits or are simply a consequence of the usual physical activities, and associated trauma, during growth. Therefore, we examined whether a recent DFF, resulting from mild or moderate trauma, is related to deficits in bone strength and cortical and trabecular bone macro- and microstructure compared with nonfracture controls. High-resolution peripheral quantitative computed tomography was used to assess micro-finite element-derived bone strength (ie, failure load) and to measure cortical and trabecular bone parameters at the distal radius and tibia in 115 boys and girls with a recent (<1 year) DFF and 108 nonfracture controls aged 8 to 15 years. Trauma levels (mild versus moderate) were assigned based on a validated classification scheme. Compared with sex-matched controls, boys and girls with a mild-trauma DFF (eg, fall from standing height) showed significant deficits at the distal radius in failure load (-13% and -11%, respectively; p < 0.05) and had higher ("worse") fall load-to-strength ratios (both +10%; p < 0.05 for boys and p = 0.06 for girls). In addition, boys and girls with a mild-trauma DFF had significant reductions in cortical area (-26% and -23%, respectively; p < 0.01) and cortical thickness (-14% and -13%, respectively; p < 0.01) compared with controls. The skeletal deficits in the mild-trauma DFF patients were generalized, as similar changes were present at the distal tibia. By contrast, both boys and girls with a moderate-trauma DFF (eg, fall from a bicycle) had virtually identical values for all of the measured bone parameters compared with controls. In conclusion, DFFs during growth have two distinct etiologies: those owing to underlying skeletal deficits leading to fractures with mild trauma versus those owing to more significant trauma in the setting of normal bone strength.
Keywords: BONE STRUCTURE; CHILDREN; FOREARM FRACTURE; HRpQCT; TRAUMA LEVELS.
© 2014 American Society for Bone and Mineral Research.
Conflict of interest statement
All authors state that they have no conflicts of interest.
Figures
Comment in
-
Increasing wrist fracture rates in children may have major implications for future adult fracture burden.Acta Orthop. 2016 Jun;87(3):296-300. doi: 10.3109/17453674.2016.1152855. Epub 2016 Feb 24. Acta Orthop. 2016. PMID: 26905618 Free PMC article.
References
-
- Landin LA. Fracture patterns in children. Analysis of 8,682 fractures with special reference to incidence, etiology and secular changes in a Swedish urban population 1950–1979. Acta Orthop Scand. 1983;202(Suppl):1–109. - PubMed
-
- Kramhoft M, Bodtker S. Epidemiology of distal forearm fractures in Danish children. Acta Orthop Scand. 1988;59:557–559. - PubMed
-
- Bailey DA, Wedge JH, McCulloch RG, Martin AD, Bernhardson SC. Epidemiology of fractures of the distal end of the radius in children as associated with growth. J Bone Joint Surg. 1989;71-A(1):1225–1231. - PubMed
-
- Cooper C, Dennison EM, Leufkens HG, Bishop N, van Staa TP. Epidemiology of childhood fractures in Britain: a study using the general practice research database. J Bone Miner Res. 2004;19(12):1976–1981. - PubMed
-
- Khosla S, Melton LJ, III, Dekutoski MB, Achenbach SJ, Oberg AL, Riggs BL. Incidence of childhood distal forearm fractures over 30 years: a population-based study. JAMA. 2003;290(11):1479–1485. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
