

Predicting risk of emergency admission to hospital using primary care data: derivation and validation of QAdmissions score
- PMID: 23959760
- PMCID: PMC3753502
- DOI: 10.1136/bmjopen-2013-003482
Predicting risk of emergency admission to hospital using primary care data: derivation and validation of QAdmissions score
Abstract
Objective: To develop and externally validate a risk algorithm (QAdmissions) to estimate the risk of emergency hospital admission for patients aged 18-100 years in primary care.
Design: Prospective open cohort study using routinely collected data from general practice linked to hospital episode data during the 2-year study period 1 January 2010 to 31 December 2011.
Setting: 405 general practices in England contributing to the national QResearch database to develop the algorithm. Two validation cohorts to validate the algorithm (1) 202 different QResearch practices and (2) 343 practices in England contributing to the Clinical Practice Research DataLink (CPRD). All general practices had data linked to hospital episode statistics at the individual patient level.
Participants: We studied 2 849 381 patients aged 18-100 years in the derivation cohort with over 4.6 million person-years of follow-up. 265 573 of these patients had one or more emergency admissions during follow-up. For the QResearch validation cohort, we identified 1 340 622 patients aged 18-100 years with over 2.2 million person-years of follow-up. Of these patients, 132 723 had one or more emergency admissions during follow-up. The CPRD cohort included 2 475 360 patients aged 18-100 years with over 3.8 million person-years of follow-up. 234 204 of these patients had one or more emergency admissions during follow-up. We excluded patients without a valid NHS number and a valid Townsend score.
Endpoint: First (ie, incident) emergency admission to hospital in the next 2 years as recorded on the linked hospital episodes records.
Risk factors: Candidate variables recorded on the general practitioner computer system including (1) demographic variables (age, sex, strategic health authority, Townsend deprivation score, ethnicity); (2) lifestyle variables (smoking, alcohol intake); (3) chronic diseases; (4) prescribed medication; (5) clinical values (body mass index, systolic blood pressure); (6) laboratory test results (haemoglobin, platelets, erythrocyte sedimentation rate, ratio of total serum cholesterol to high density lipoprotein cholesterol concentrations, liver function tests). We also included the number of emergency admissions in the preceding year based on information recorded on the linked hospital episodes records.
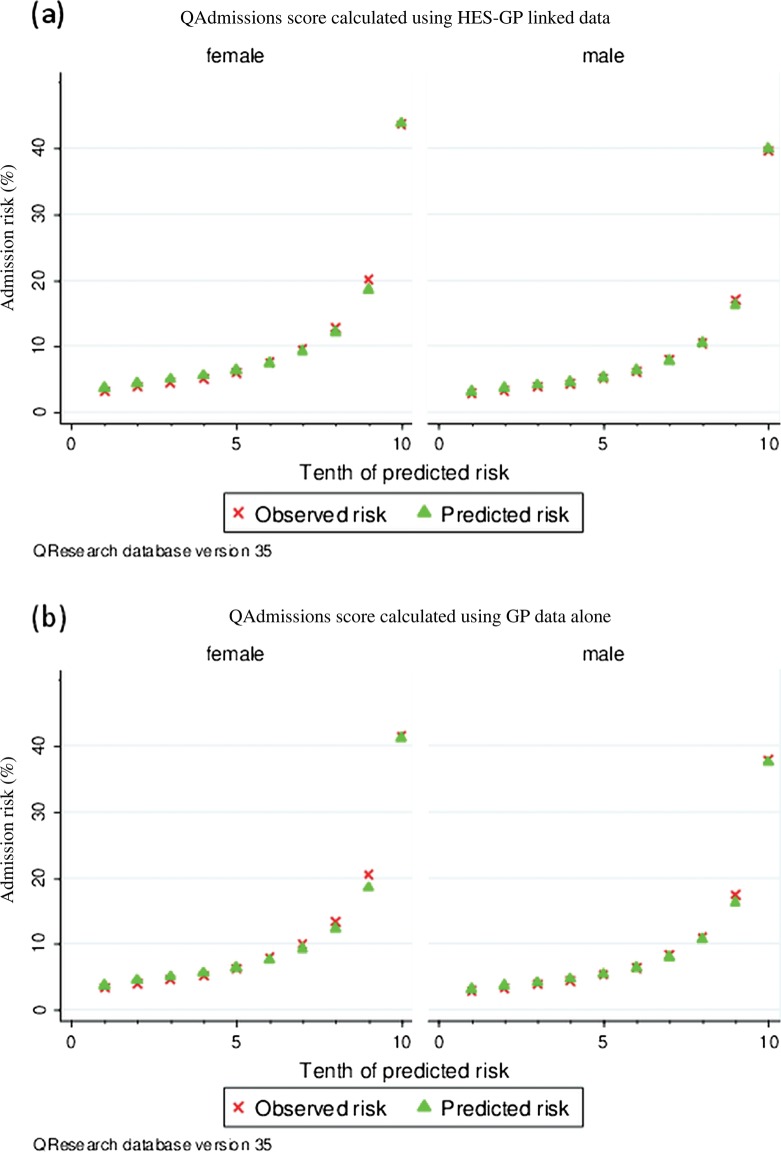
Results: The final QAdmissions algorithm incorporated 30 variables. When applied to the QResearch validation cohort, it explained 41% of the variation in women and 43% of that in men. The D statistic for QAdmissions was 1.7 in women and 1.8 in men. The receiver operating curve statistic was 0.78 for men and 0.77 for women. QAdmissions had good performance on all measures of discrimination and calibration. The positive predictive value for emergency admissions for the top tenth of patients at highest risk was 42% and the sensitivity was 39%. The results for the CPRD validation cohort were similar.
Conclusions: The QAdmissions model provided a valid measure of absolute risk of emergency admission to hospital in the general population as shown by its performance in a separate validation cohort. Further research is needed to evaluate the cost-effectiveness of using these algorithms in primary care.
Keywords: EPIDEMIOLOGY; PREVENTIVE MEDICINE; PRIMARY CARE.
Figures
References
-
- Lewis G, Curry N, Bardsley M. Choosing a predictive risk model: a guide for commissioners in England. Nuffield trust, 2011:20
-
- NHS England Enhanced service specification: Risk profiling and care management scheme. Secondary Enhanced service specification: risk profiling and care management scheme 2013. http://www.england.nhs.uk/wp-content/uploads/2013/03/ess-risk-profiling.pdf
-
- ISD Scotland Scottish Patients at Risk of Readmission and Admission (SPARRA)—a report on the development of SPARRA. Secondary Scottish Patients at Risk of Readmission and Admission (SPARRA)—a report on the development of SPARRA 2011. http://www.isdscotland.org/Health-Topics/Health-and-Social-Community-Car...
LinkOut - more resources
Full Text Sources
Other Literature Sources