

What role do plain radiographs have in assessing the skeletally immature acromioclavicular joint?
- PMID: 23959906
- PMCID: PMC3889446
- DOI: 10.1007/s11999-013-3242-x
What role do plain radiographs have in assessing the skeletally immature acromioclavicular joint?
Abstract
Background: Because of incomplete ossification of the coracoid process and acromion, acromioclavicular joint configuration in the skeletally immature patient differs from that of adults. Although comparison to radiographic standards for this joint is critical in the evaluation of acromioclavicular joint injuries, these standards are not well defined for children or adolescents.
Questions/purposes: We therefore sought to determine (1) the reliability of numerous radiographic measurements of the skeletally immature acromioclavicular joint, including the vertical and shortest coracoclavicular interval, and the acromioclavicular joint offset; (2) the timing of ossification of the acromion and coracoid in males and females; and (3) the differences in the values of these radiographic measurements based on age and sex.
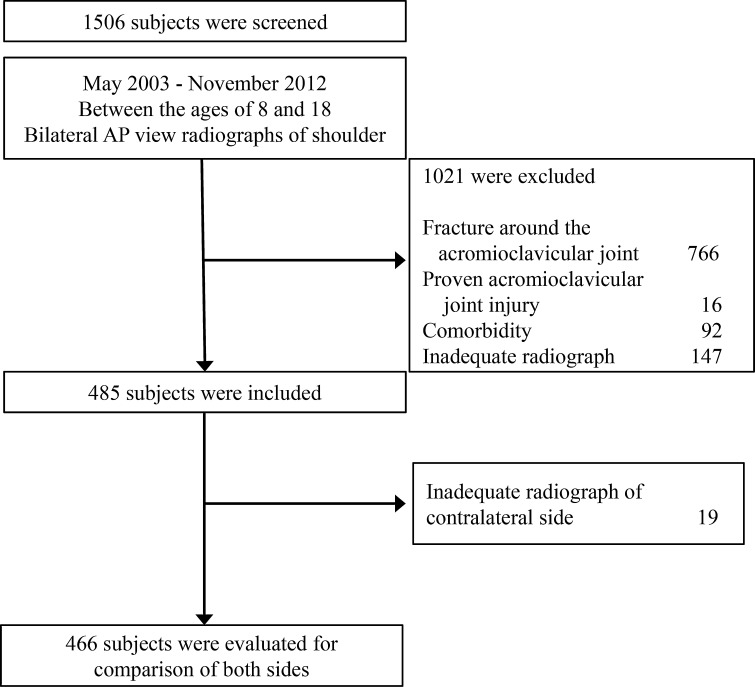
Methods: This study was based on a total of 485 subjects, 8 to 18 years old, who underwent conventional AP view radiographs of both shoulders. The 485 subjects were included to assess normal configuration around the acromioclavicular joint and 466 of these subjects were evaluated for comparison between both sides. The vertical and shortest coracoclavicular interval, coracoclavicular clavicle width ratio, acromioclavicular joint offset, and difference of the coracoclavicular interval of both sides were measured. A reliability test was conducted before obtaining the main measurements. The relationship of measurements with sex, age, and stage of ossification was evaluated.
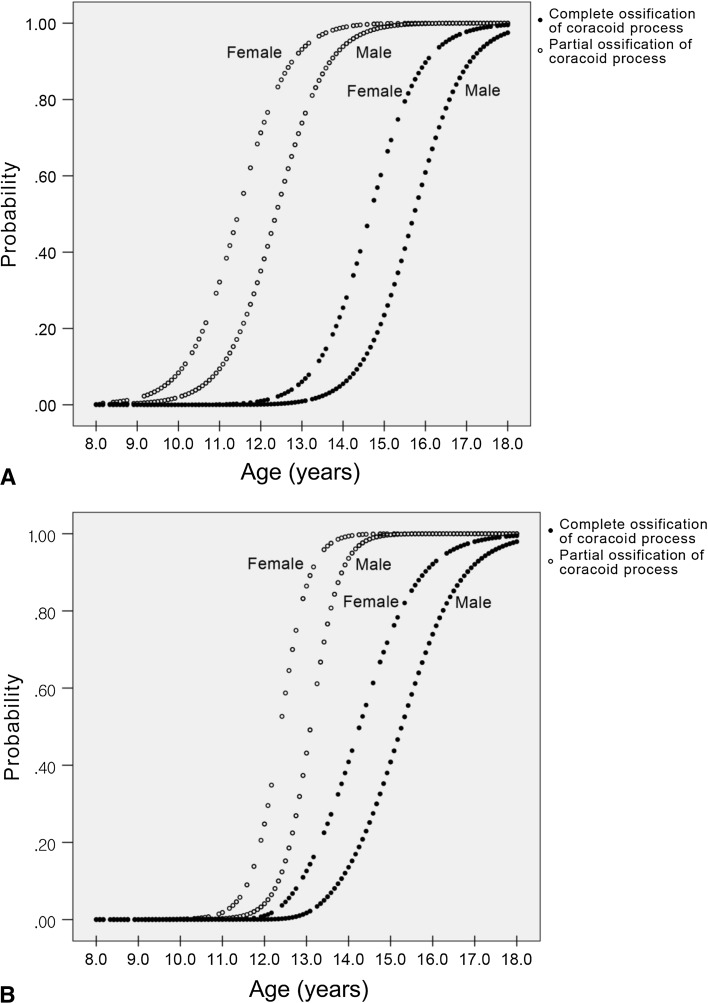
Results: The vertical and shortest coracoclavicular interval showed excellent reliability (intraclass correlation coefficient ([ICC], 0.918 and 0.934). The acromioclavicular joint offset showed low reliability (ICC, 0.543). The ossification centers of the acromion and the coracoid processes appeared and fused earlier in females than in males. The vertical coracoclavicular interval, which was not affected by partial ossification of the coracoid process, was less than 11 mm in the 90% quantile of total subjects in males and 10 mm in the 90% quantile in females. The difference of the vertical coracoclavicular interval of both sides was less than 50% in 436 of 466 (93.4%) patients.
Conclusions: The vertical coracoclavicular interval was the best parameter to assess acromioclavicular joint dislocation in skeletally immature patients. Comparison of both sides of the acromioclavicular joint could help to inform physicians in predicting the need for additional evaluations.
Figures



References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
