

Acute kidney injury in statin initiators
- PMID: 23960024
- PMCID: PMC3822439
- DOI: 10.1002/pds.3500
Acute kidney injury in statin initiators
Abstract
Purpose: Statins are widely used for preventing cardiovascular disease, yet recent reports suggest an increased risk of acute kidney injury (AKI). We estimated the one-year risk of AKI associated with statin initiation and determined the comparative safety of individual statin formulations.
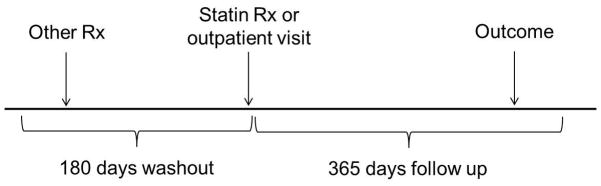
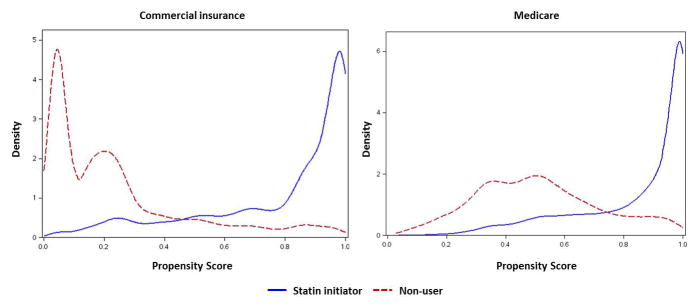
Methods: We performed a cohort study in insurance billing data from commercial and Medicare insurance plans in the United States for the years 2000-2010. We identified statin initiators and non-users with histories of medication use and healthcare utilization. AKI diagnosis codes were identified in the one year following the index date. We estimated hazard ratios (HR) and 95% confidence intervals (CI) with adjusted and propensity score (PS)-matched Cox-proportional hazards models. Models were run separately in insurance groups and adjusted for cardiovascular and renal risk factors, markers of healthcare utilization, and other medication use.
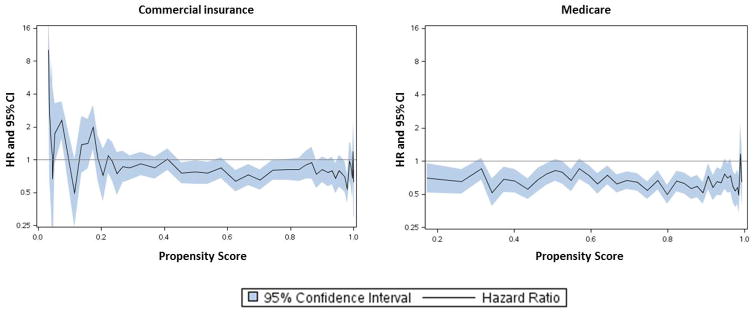
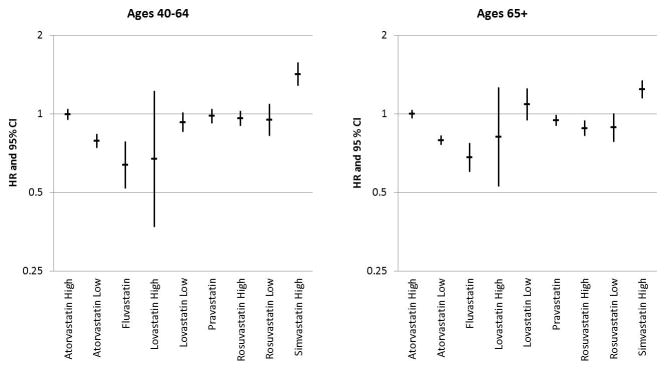
Results: We identified 3,905,155 statin initiators and 2,817,621 eligible non-users. The adjusted HR of AKI in statin initiators compared to non-users was: commercial, HR = 1.04 (95% CI: 0.99, 1.09); Medicare, HR = 0.72 (95% CI: 0.70, 0.75). PS-matching yielded: commercial, HR = 0.82 (95% CI: 0.78, 0.87); Medicare, HR = 0.66 (95% CI: 0.63, 0.69). As individual formulations, higher-potency simvastatin was associated with an increased risk of AKI over lower-potency simvastatin in adjusted models: commercial, HR = 1.42 (95% CI: 1.28, 1.58); Medicare, HR = 1.24 (95% CI: 1.15, 1.35).
Conclusions: As a class, statin initiation was not associated with an increase in AKI. However, higher-potency simvastatin did exhibit an increased AKI risk.
Keywords: acute kidney injury; comparative effectiveness; drug safety; pharmacoepidemiology; propensity scores.
Copyright © 2013 John Wiley & Sons, Ltd.
Conflict of interest statement
Dr. Brookhart has served on scientific advisory boards for Pfizer, with honoraria either donated to charity or received by UNC.
Dr. Simpson has received research support from Merck, and honoraria for lectures from Merck and Pfizer.
Dr. Jonsson Funk: GlaxoSmithKline (GSK) has a collaborative agreement with the Center for Pharmacoepidemiology, Department of Epidemiology, UNC Chapel Hill. GSK does not review any research nor provide any input into the analysis of the drug classes being studied.
Dr. Stürmer receives investigator-initiated research funding and support as Principal Investigator (RO1 AG023178) and Co-Investigator (RO1 AG018833) from the National Institute on Aging at the National Institutes of Health. He also receives research funding as Principal Investigator of the UNC-DEcIDE center from the Agency for Healthcare Research and Quality. Dr. Stürmer does not accept personal compensation of any kind from any pharmaceutical company, though he receives salary support from the Center for Pharmacoepidemiology in the Department of Epidemiology at UNC and from unrestricted research grants from pharmaceutical companies to UNC.
Similar articles
-
Statin use and the risk of acute kidney injury in older adults.BMC Nephrol. 2019 Mar 25;20(1):103. doi: 10.1186/s12882-019-1280-7. BMC Nephrol. 2019. PMID: 30909872 Free PMC article.
-
Use of high potency statins and rates of admission for acute kidney injury: multicenter, retrospective observational analysis of administrative databases.BMJ. 2013 Mar 18;346:f880. doi: 10.1136/bmj.f880. BMJ. 2013. PMID: 23511950
-
Simvastatin dose and acute kidney injury without concurrent serious muscle injury: A nationwide nested case-control study.PLoS One. 2017 Jul 28;12(7):e0182066. doi: 10.1371/journal.pone.0182066. eCollection 2017. PLoS One. 2017. PMID: 28753656 Free PMC article.
-
Comparative risk of lipophilic and hydrophilic statins on incident depression: A retrospective cohort study.J Affect Disord. 2018 Oct 1;238:542-546. doi: 10.1016/j.jad.2018.06.021. Epub 2018 Jun 15. J Affect Disord. 2018. PMID: 29936394
-
Efficacy of Short-Term Statin Treatment for the Prevention of Contrast-Induced Acute Kidney Injury in Patients Undergoing Coronary Angiography/Percutaneous Coronary Intervention: A Meta-Analysis of 21 Randomized Controlled Trials.Am J Cardiovasc Drugs. 2016 Jun;16(3):201-19. doi: 10.1007/s40256-016-0164-5. Am J Cardiovasc Drugs. 2016. PMID: 26899537 Review.
Cited by
-
Antimuscarinic use and discontinuation in an older adult population.Arch Gerontol Geriatr. 2019 Jan-Feb;80:1-11. doi: 10.1016/j.archger.2018.09.005. Epub 2018 Sep 22. Arch Gerontol Geriatr. 2019. PMID: 30268971 Free PMC article.
-
Comparative effectiveness research and its utility in In-clinic practice.Perspect Clin Res. 2016 Jan-Mar;7(1):9-14. doi: 10.4103/2229-3485.173780. Perspect Clin Res. 2016. PMID: 26955571 Free PMC article. Review.
-
Hypernatremia is a significant risk factor for acute kidney injury after subarachnoid hemorrhage: a retrospective analysis.Neurocrit Care. 2015 Apr;22(2):184-91. doi: 10.1007/s12028-014-0067-8. Neurocrit Care. 2015. PMID: 25231531
-
Effects of statins on the incidence and outcomes of acute kidney injury in critically ill patients: a systematic review and meta-analysis.Arch Med Sci. 2023 Jan 27;19(4):952-964. doi: 10.5114/aoms/159992. eCollection 2023. Arch Med Sci. 2023. PMID: 37560738 Free PMC article. Review.
-
Statin use and the risk of acute kidney injury in older adults.BMC Nephrol. 2019 Mar 25;20(1):103. doi: 10.1186/s12882-019-1280-7. BMC Nephrol. 2019. PMID: 30909872 Free PMC article.
References
-
- Spatz ES, Canavan ME, Desai MM. From here to JUPITER: identifying new patients for statin therapy using data from the 1999–2004 National Health and Nutrition Examination Survey. Circulation Cardiovascular quality and outcomes. 2009;2:41–8. - PubMed
-
- Lin V, Holman JR. Which drugs should post-MI patients routinely receive? The Journal of Family Practice. 2010;59:527–9. - PubMed
-
- Mills EJ, Wu P, Chong G, et al. Efficacy and safety of statin treatment for cardiovascular disease: a network meta-analysis of 170,255 patients from 76 randomized trials. QJM: monthly journal of the Association of Physicians. 2011;104:109–24. - PubMed
-
- Albert MA, Danielson E, Rifai N, Ridker PM. Effect of statin therapy on C-reactive protein levels: the pravastatin inflammation/CRP evaluation (PRINCE): a randomized trial and cohort study. JAMA: the journal of the American Medical Association. 2001;286:64–70. - PubMed
-
- Giusti-Paiva A, Martinez MR, Felix JV, et al. Simvastatin decreases nitric oxide overproduction and reverts the impaired vascular responsiveness induced by endotoxic shock in rats. Shock. 2004;21:271–5. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
