

Classification of relapse pattern in clubfoot treated with Ponseti technique
- PMID: 23960281
- PMCID: PMC3745691
- DOI: 10.4103/0019-5413.114921
Classification of relapse pattern in clubfoot treated with Ponseti technique
Abstract
Background: Relapse of clubfoot deformity following correction by Ponseti technique is not uncommon. The relapsed feet progress from flexible to rigid if left untreated and can become as severe as the initial deformity. No definitive classification exists to assess a relapsed clubfoot. Some authors have used the Pirani score to rate the relapse while others have used descriptive terms. The purpose of this study is to analyze the relapse pattern in clubfeet that have undergone treatment with the Ponseti method and propose a simple classification for relapsed clubfeet.
Materials and methods: Ninety-one children (164 feet) with idiopathic clubfeet who underwent treatment with Ponseti technique presented with relapse of the deformity. There were 68 boys and 23 girls. Mean age at presentation for casting was 10.71 days (range 7-22 days). Seventy three children (146 feet, 80%) had bilateral involvement and 18 (20%) had unilateral clubfeet. The mean Pirani Score was 5.6 and 5.5 in bilateral and unilateral groups respectively. Percutaneous heel cord tenotomy was done in 65 children (130 feet, 89%) in the bilateral group and in 12 children (66%) with unilateral clubfoot.
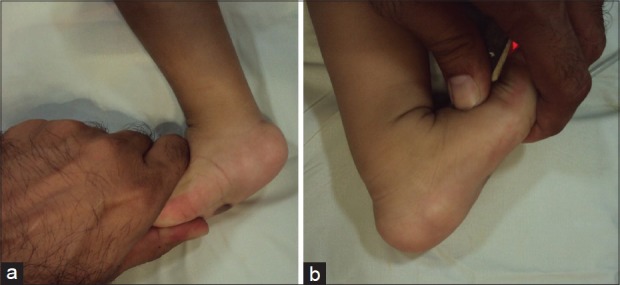
Results: Five relapse patterns were identified at a mean followup of 4.5 years (range 3-5 years) which forms the basis of this study. These relapse patterns were classified as: Grade IA: decrease in ankle dorsiflexion from15 degrees to neutral, Grade IB: dynamic forefoot adduction or supination, Grade IIA - rigid equinus, Grade IIB - rigid adduction of forefoot/midfoot complex and Grade III: combination of two or more deformities: Fixed equinus, varus and forefoot adduction. In the bilateral group, 21 children (38 feet, 28%) had Grade IA relapse. Twenty four children (46 feet, 34%) had dynamic intoeing (Grade IB) on walking. Thirteen children (22 feet, 16%) had true ankle equinus of varying degress (Grade IIA); eight children (13 feet, 9.7%) had fixed adduction deformity of the forefoot (Grade IIB) and seven children (14 feet, 10.7%) had two or more fixed deformities. In the unilateral group seven cases (38%) had reduced dorsiflexion (Grade IA), six (33%) had dynamic adduction (Grade IB), two (11%) had fixed equinus and adduction respectively (Grade IIA and IIB) and one (5%) child had fixed equinus and adduction deformity (Grade III). The relapses were treated by full time splint application, re-casting, tibialis anterior transfer, posterior release, corrective lateral closing wedge osteotomy and a comprehensive subtalar release. Splint compliance was compromised in both groups.
Conclusion: Relapse pattern in clubfeet can be broadly classified into three distinct subsets. Early identification of relapses and early intervention will prevent major soft tissue surgery. A universal language of relapse pattern will allow comparison of results of intervention.
Keywords: Classification; Ponseti technique; clubfoot; relapse.
Conflict of interest statement
Figures



References
-
- Ponseti IV. Current concepts review: Treatment of congenital clubfoot. J Bone Joint Surg Am. 1992;74:448–54. - PubMed
-
- Ponseti IV, Smoley EN. Congenital club foot: The results of treatment. J Bone Joint Surg Am. 1963;45:261–75.
-
- Owen RM, Kembhavi G. A critical review of interventions for clubfoot low and middle income countries: Effectiveness and contextual influences. J Pediatr Orthop. 2012;21:59–67. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources