

doi: 10.1016/j.sjopt.2010.10.012.
Epub 2010 Oct 18.
Dacryocystorhinostomy: History, evolution and future directions
Affiliations
- PMID: 23960901
- PMCID: PMC3729489
- DOI: 10.1016/j.sjopt.2010.10.012
Item in Clipboard
Dacryocystorhinostomy: History, evolution and future directions
Saudi J Ophthalmol.
2011 Jan.
Abstract
Dacryocystorhinostomy (DCR) is a procedure of choice for nasolacrimal duct obstruction and chronic dacryostenosis in the setting of patent canaliculi and a functional lacrimal pump. Two major approaches are utilized: external, via a transcutaneous incision and endonasal endoscopically guided. The surgery has a high success rate via both approaches. We review the history, evolution, current techniques, complications and future directions of DCR.
Keywords: Dacryocystorhinostomy, Endoscopic dacryocystorhinostomy, Balloon dacryoplasty, Dacryocystitis, Nasolacrimal duct obstruction.
Figures

Acute and chronic dacryocystitis and lacrimal sac abscess. (A) A grossly distended, tender left lacrimal sac abscess is seen. Note chronically distended right lacrimal sac (∗). (B) Immediately after office based incision and drainage of the left lacrimal sac abscess. The mucopurulent material was cultured and revealed methcillin-resistant Staphylococcus aureus (MRSA). The patient was treated medically and underwent an uncomplicated external DCR on the left followed 1–2 months later by an external DCR on the right.
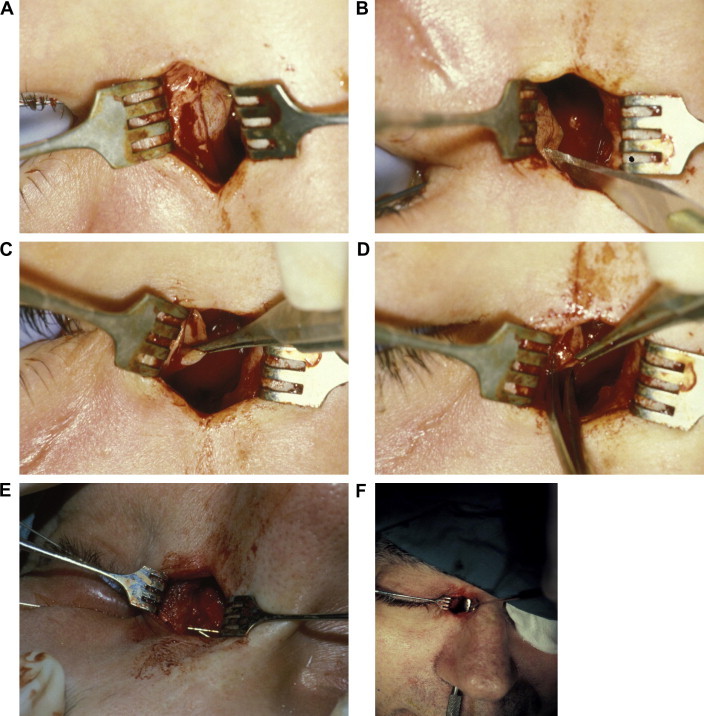
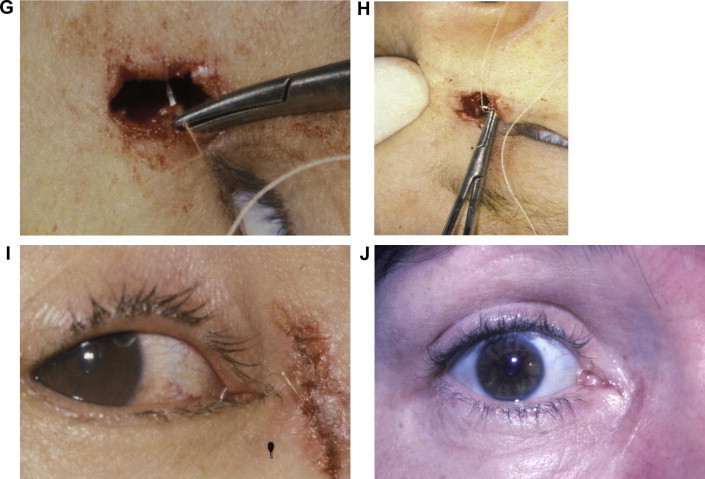
Key steps in external DCR. (A) Tenting of lacrimal sac wall with Bowman probe. (B) Incision into lacrimal sac with #11 Bard-Parker blade. (C & D). Posterior flap is grasped and excised. (E) Bowman probes passed through upper and lower canaliculi demonstrating a common internal punctum. (F) The bony ostium is demonstrated with Freer elevator passed up through the nose. (G) Suturing the anterior sac flap to anterior nasal mucosal flap with 5-0 polyglactin suture on P2 needle. (H) Surgeon’s view. (I) Immediate postoperative appearance. Skin is closed with interrupted 6-0 plain suture. Crawford tube is in place. (J) Six week postoperative appearance prior to tube removal. A faint incision line without scar hypertrophy or webbing is noted.
Key steps in external DCR. (A) Tenting of lacrimal sac wall with Bowman probe. (B) Incision into lacrimal sac with #11 Bard-Parker blade. (C & D). Posterior flap is grasped and excised. (E) Bowman probes passed through upper and lower canaliculi demonstrating a common internal punctum. (F) The bony ostium is demonstrated with Freer elevator passed up through the nose. (G) Suturing the anterior sac flap to anterior nasal mucosal flap with 5-0 polyglactin suture on P2 needle. (H) Surgeon’s view. (I) Immediate postoperative appearance. Skin is closed with interrupted 6-0 plain suture. Crawford tube is in place. (J) Six week postoperative appearance prior to tube removal. A faint incision line without scar hypertrophy or webbing is noted.
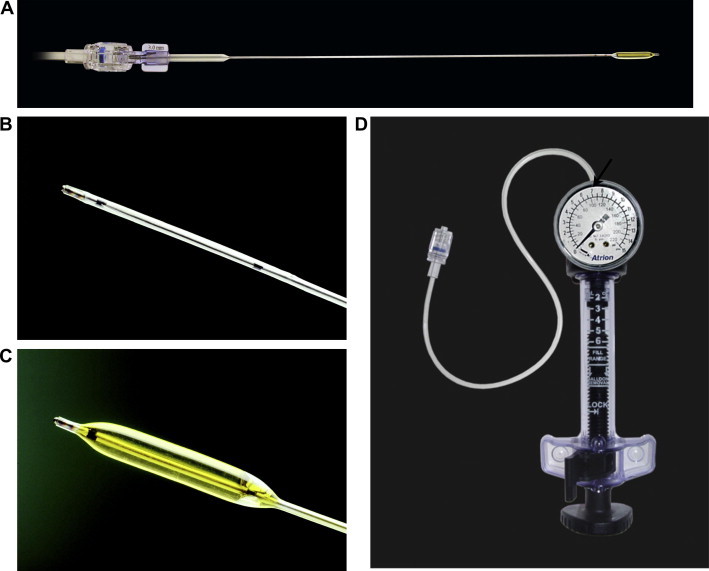
Balloon dacryoplasty apparatus. (A) 3 mm (diameter) balloon (expanded). (B) Balloon tip in a deflated state. (C) Balloon tip inflated. (D) The pump apparatus with gauge. Arrow indicates the 7 atm mark. Photos courtesy of Quest Medical, Inc., Allen, TX, USA.
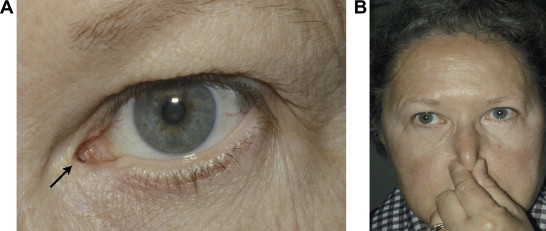
(A) A well positioned Jones tube is demonstrated (arrow). (B) Daily maintenance of Jones tube. After instilling 2–3 drops of artificial tears forced inspiration through the nose with the nose occluded is performed.
References
-
- Agarwal S. Endoscopic dacryocystorhinostomy for acquired nasolacrimal duct obstruction. J. Laryngol. Otol. 2009;123:1226–1228. - PubMed
-
- Ajit R., Inkster C., Tuck J., Mortzos P. Orbital emphysema: an unusual complication of balloon dacryocystoplasty. Br. J. Radiol. 2004;77(924):1057–1058. - PubMed
-
- Anari S., Ainsworth G., Robson A.K. Cost-efficiency of endoscopic and external dacryocystorhinostomy. J. Laryngol. Otol. 2008;122:476–479. - PubMed
-
- Badilla J., Dolman P.J. Cerebrospinal fluid leaks complicating orbital or oculoplastic surgery. Arch. Ophthalmol. 2007;125(12):1631–1634. - PubMed
-
- Baldeschi L., Macandie K., Hintschich C.R. The length of unsutured mucosal margins in external dacryocystorhinostomy. Am. J. Ophthalmol. 2004;138(5):840–844. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
