

doi: 10.1016/j.sjopt.2010.10.009.
Epub 2010 Oct 13.
Reconstructive options for the medial canthus and eyelids following tumor excision
Affiliations
- PMID: 23960904
- PMCID: PMC3729517
- DOI: 10.1016/j.sjopt.2010.10.009
Item in Clipboard
Reconstructive options for the medial canthus and eyelids following tumor excision
Saudi J Ophthalmol.
2011 Jan.
Abstract
General principles provide the framework for eyelid and periorbital reconstruction following tumor excision. Eyelid tumors involving the medial canthus region and/or lacrimal system add to the complexity of reconstructive planning. The nature of the tumor, patient and tissue factors, and surgeon preference guide repair design choices. Reconstructive considerations and options following medial canthal tumor resection are described.
Keywords: Flap; Graft; Medial canthus; Reconstruction; Tumor.
Figures
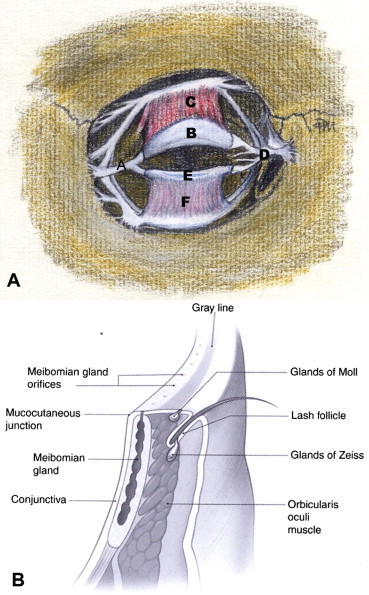
(A) Anterior view of deeper eyelid and periorbital structures: (A) lateral canthal tendon; (B) upper eyelid tarsus; (C) levator aponeurosis; (D) medial canthal tendon; (E) lower eyelid tarsus; (F) lower eyelid retractors (illustration by Trish Michels). (B) Cross-section of the eyelid margin anatomy.
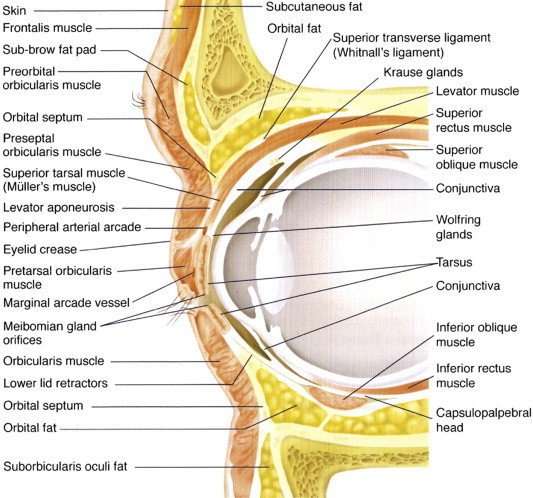
Cross-section of the orbital and periorbital anatomy.
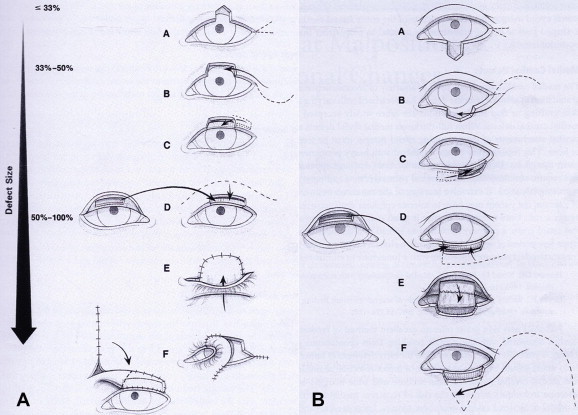
(A) Reconstructive options for upper eyelid defects: (A) direct primary closure with or without canthotomy and cantholysis; (B) direct primary closure with canthotomy/cantholysis and semicircular flap; (C) adjacent tarsoconjunctival flap with FTSG (FTSG not drawn); (D) free tarsoconjuctival graft and skin–muscle flap; (E) Cutler–Beard full-thickness lower eyelid advancement flap; (F) lower eyelid switch flap; (G) glabellar/median forehead flap with free tarsoconjunctival graft. (B) Reconstructive options for lower eyelid defects: (A) direct primary closure with or without canthotomy and cantholysis; (B) direct primary closure with canthotomy/cantholysis and semicircular flap; (C) adjacent tarsoconjunctival flap with FTSG; (D) free tarsoconjunctival graft and skin–muscle flap; (E) Hughes upper eyelid tarsoconjunctival flap and FTSG (FTSG not drawn); (F) Mustardè flap with free tarsoconjunctival graft.
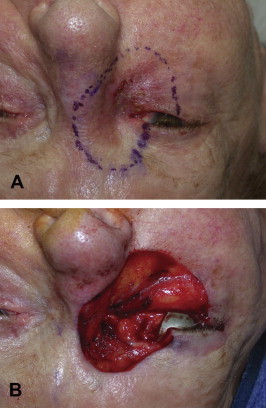
(A) Preoperative photograph of an 88-year-old female with biopsy confirmed melanoma of the right medial canthus. The excision margins have been marked with a 5 mm border surrounding the lesion. The margins include the entire medial canthus, greater than 50% of the lower lid, 33–50% of the upper lid, and lacrimal systems of both upper and lower eyelids. Portions of the brow, nose, and cheek are also encompassed within the resection margins. (B) Intraoperative photograph of the resulting defect immediately following excision of the tumor detailed in (A). The depth of the resection was to bare sclera and continued medially on the surface of the medial canthal tendon to the lateral nasal wall. Dissection was continued superiorly and inferiorly to the included portions of the brow and cheek, respectively. All tissues anterior to periosteum were removed.
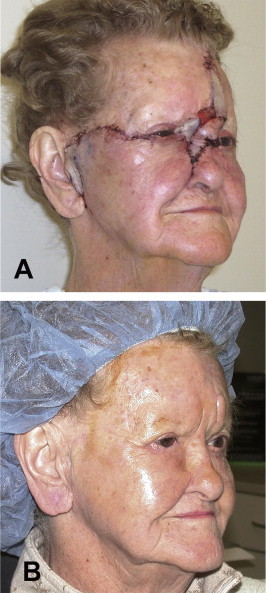
(A) Postoperative Day 1. The lower eyelid was reconstructed with a free tarsoconjunctival graft (posterior lamella) from the contralateral upper lid and a Mustardè flap (anterior lamella). The upper eyelid was reapproximated to the medial canthal tendon following a lateral canthotomy/cantholysis. A glabellar flap was rotated inferior to the lateral nasal wall and a portion of the medial canthus. Telfa gauze is placed under the flap bridge in anticipation for subsequent reversal. A FTSG was harvested from the patient’s left clavicular area and portioned to supply graft material to the preauricular, medial canthal, and forehead regions. The lacrimal system was not addressed secondary to the nature of the tumor. (B) Postoperative Day 136. All original flaps and grafts remain viable and no tumor recurrence is noted. The glabellar flap has previously been reversed. The raised island of tissue above the left brow was thinned at this visit. Lid margins are in good alignment and there was no indication of ocular exposure.
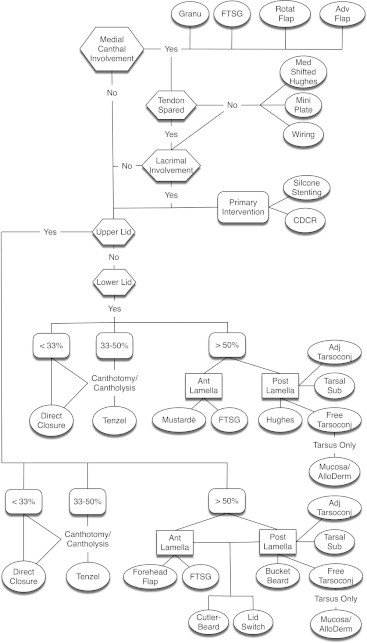
Decision tree outlining surgical design options for upper and lower lid reconstruction with or without medical canthal, tendinous, and/or lacrimal involvement.
References
-
- Chao, Y., Xin, X., Jiangping, C., 2009. Medial canthal reconstruction with combined glabellar and orbicularis oculi myocutaneous advancement flaps. J. Plast. Reconstr. Aesthet. Surg. (published online ahead of print December 1, 2009). - PubMed
-
- Collin J.R.O. third ed. Butterworth–Heinemann; Oxford: 2006. A Manual of Systematic Eyelid Surgery. pp. 16–23.
-
- Collin J.R.O. third ed. Butterworth–Heinemann; Oxford: 2006. A Manual of Systematic Eyelid Surgery. p. 149.
-
- Collin J.R.O. third ed. Butterworth–Heinemann; Oxford: 2006. A Manual of Systematic Eyelid Surgery. pp. 115–145.
-
- Doxanas M.T., Anderson R.L. Clinical Orbital Anatomy. Williams & Wilkins; Baltimore: 1984. Eyebrows, eyelids, and anterior orbit; pp. 57–88.
LinkOut - more resources
Full Text Sources
