

Healed corneal ulcer with keloid formation
- PMID: 23961000
- PMCID: PMC3729576
- DOI: 10.1016/j.sjopt.2011.10.005
Healed corneal ulcer with keloid formation
Abstract
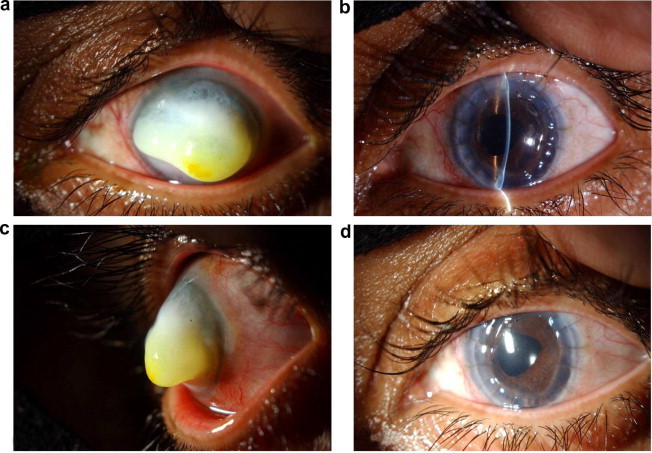
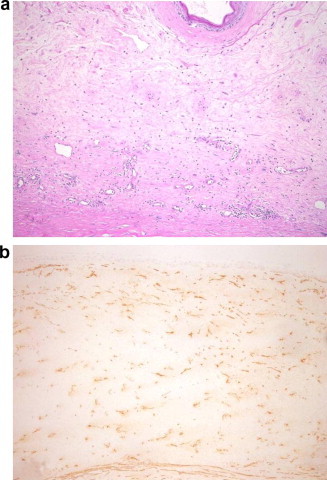
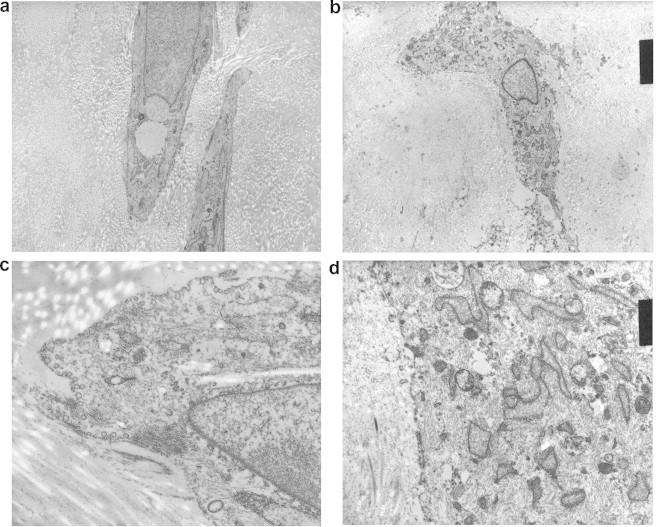
We are reporting a 34-year-old Arabic white female patient who presented with a white mass covering her left cornea following multiple ocular surgeries and healed corneal ulcer. The lesion obscured further view of the iris, pupil and lens. The patient underwent penetrating keratoplasty and the histopathologic study of the left corneal button showed epithelial hyperplasia, absent Bowman's layer and subepithelial fibrovascular proliferation. The histopathologic appearance was suggestive of a corneal keloid which was supported by further ultrastructural study. The corneal graft remained clear 6 months after surgery and the patient was satisfied with the visual outcome. Penetrating keratoplasty may be an effective surgical option for corneal keloids in young adult patients.
Keywords: Corneal mass; Histopathology; Keloid; Penetrating keratoplasty.
Figures
References
-
- Cibis G.W., Tripathi R.C., Tripathi B.J., Harris D.J. Corneal keloid in Lowe’s syndrome. Arch Ophthalmol. 1982;100:1795–1799. - PubMed
-
- Esquenazi S., Eustis H.S., Bazan H.E., Leon A., He J. Corneal keloid in Lowe syndrome. J Pediatr Ophthalmol Strabismus. 2005;42:308–310. - PubMed
-
- Shoukrey N.M., Tabbara K.F. Ultrastructural study of a corneal keloid. Eye (Lond) 1993;7(Pt 3):379–387. - PubMed
LinkOut - more resources
Full Text Sources
