

doi: 10.1016/j.sjopt.2012.08.009.
Fungal rhinosinusitis and imaging modalities
Affiliations
- PMID: 23961027
- PMCID: PMC3729552
- DOI: 10.1016/j.sjopt.2012.08.009
Item in Clipboard
Fungal rhinosinusitis and imaging modalities
Saudi J Ophthalmol.
2012 Oct.
Abstract
This report provides an overview of fungal rhinosinusitis with a particular focus on acute fulminant invasive fungal sinusitis (AFIFS). Imaging modalities and findings that aid in diagnosis and surgical planning are reviewed with a pathophysiologic focus. In addition, the differential diagnosis based on imaging suggestive of AFIFS is considered.
Keywords: Acute fulminant invasive fungal sinusitis; Computed tomography; Fungal rhinosinusitis; Imaging; Magnetic Resonance Imaging.
Figures
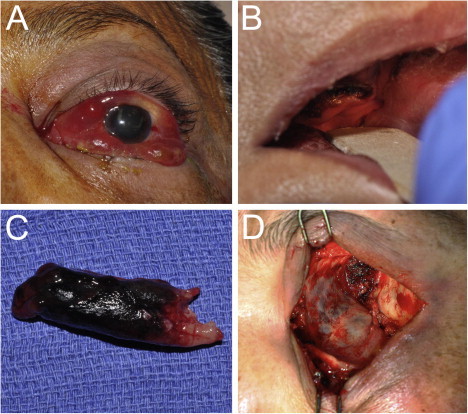
(A) 58 year-old female in diabetic ketoacidosis presents with decreased vision, chemosis, proptosis and ophthalmoplegia on the left side concerning for AFIFS. (B) Oral exam demonstrates poor dental hygiene and necrosis of the hard palate. (C) Endoscopic exam reveals necrosis of the left inferior turbinate which was removed during debridement. Tissue culture eventually grew Rhizopus microsporious. (D) Orbital exenteration was performed in conjunction with nasal and sinus debridement because of significant orbital involvement seen on imaging. Involvement of the ethmoid sinus air cells can be appreciated through the thin medial wall of the orbit.
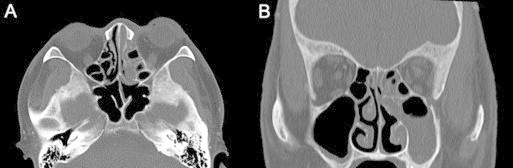
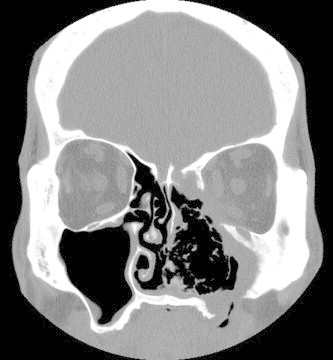
Axial (A) and coronal (B) non-enhanced CT of AFIFS shows opacification of the left ethmoid, left maxillary sinus and left nasal cavity.

Axial non-enhanced CT of AFIFS demonstrates opacification of the left maxillary sinus with soft tissue inflammation of the premalar tissues (arrowhead) and of the retroantral fat (arrow).
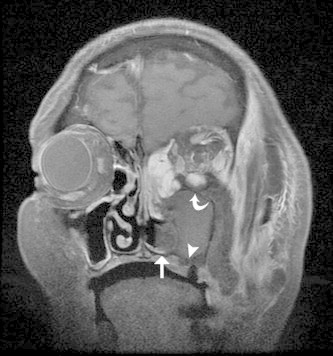
Coronal T1 MR with gadolinium and fat suppression of AFIFS shows opacification of left maxillary and ethmoid sinuses with hypointense middle and inferior turbinates (straight arrow) and loss of contrast enhancement of the maxillary mucosa (arrowhead) and inferior rectus muscle (curved arrow).
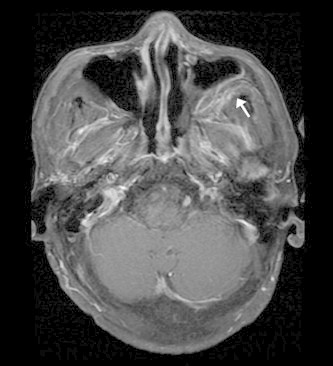
Axial T1 MR with gadolinium and fat suppression of AFIFS demonstrates enhancement of the retroantral fat (arrow).
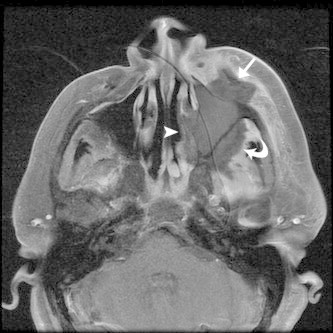
Axial T1 MR with gadolinium and fat suppression of AFIFS shows opacification of the left maxillary sinus with loss of contrast enhancement of the sinus wall, premalar tissues (straight arrow), retroantral fat (curved arrow) and of the lateral wall of the nasal cavity (arrowhead) which likely correlates to tissue necrosis.
Coronal non-enhanced CT of granulomatosis with polyangitis demonstrates a homogenous soft tissue mass extending into the left orbit with erosive changes of the left nasal cavity, ethmoid and maxillary sinuses resulting in septal perforation and bony erosion of the maxilla.

Coronal T2 MR of sinonasal squamous cell carcinoma shows a large mass involving the nasal cavity, bilateral ethmoid sinuses and left maxillary sinus with infiltration into the left orbit.

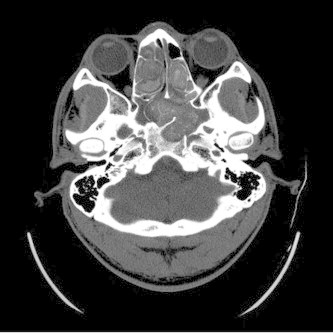
Axial CT with contrast of granulomatous invasive fungal rhinosinusitis demonstrating opacification of the ethmoid sinuses and fat stranding of the intraconal space of the right orbital apex.
Axial CT of allergic fungal rhinosinusitis shows bilateral involvement of the ethmoid and sphenoid sinuses filled with hyperintense mucin and evidence of sinus expansion and bone erosion. (Courtesy of William Dillon, MD and Songling Liu, MD.)
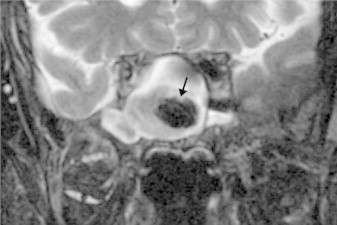
Coronal T2 MR of a fungus ball of the sphenoid sinus demonstrates low signal intensity (arrow). (Courtesy of William Dillon, MD and Songling Liu, MD.)

Similar articles
-
Computed tomography and magnetic resonance imaging characteristics of acute invasive fungal sinusitis.Arch Otolaryngol Head Neck Surg. 2011 Oct;137(10):1005-10. doi: 10.1001/archoto.2011.170. Arch Otolaryngol Head Neck Surg. 2011. PMID: 22006778
-
Usefulness of computed tomography and magnetic resonance in fulminant invasive fungal rhinosinusitis.Am J Rhinol. 2001 Jul-Aug;15(4):255-61. Am J Rhinol. 2001. PMID: 11554658
-
Invasive fungal sinusitis and complications of rhinosinusitis.Otolaryngol Clin North Am. 2008 Jun;41(3):497-524, viii. doi: 10.1016/j.otc.2008.01.001. Otolaryngol Clin North Am. 2008. PMID: 18435995 Review.
-
Chronic invasive fungal rhinosinusitis.Otolaryngol Clin North Am. 2000 Apr;33(2):375-87. doi: 10.1016/s0030-6665(00)80012-2. Otolaryngol Clin North Am. 2000. PMID: 10736411
-
Fungal Rhinosinusitis: A Radiological Review With Intraoperative Correlation.Can Assoc Radiol J. 2017 May;68(2):178-186. doi: 10.1016/j.carj.2016.12.009. Can Assoc Radiol J. 2017. PMID: 28438285 Review.
Cited by
-
Sinonasal Fungal Infections and Complications: A Pictorial Review.J Clin Imaging Sci. 2016 Jun 14;6:23. doi: 10.4103/2156-7514.184010. eCollection 2016. J Clin Imaging Sci. 2016. PMID: 27403401 Free PMC article.
-
Chronic invasive fungal sinusitis with orbital and olfactory cleft involvement secondary to indolent mucormycosis.Am J Ophthalmol Case Rep. 2022 Feb 18;26:101448. doi: 10.1016/j.ajoc.2022.101448. eCollection 2022 Jun. Am J Ophthalmol Case Rep. 2022. PMID: 35243178 Free PMC article.
-
Update in oculoplastic imaging.Saudi J Ophthalmol. 2012 Oct;26(4):347-8. doi: 10.1016/j.sjopt.2012.11.001. Epub 2012 Nov 10. Saudi J Ophthalmol. 2012. PMID: 23961018 Free PMC article. No abstract available.
-
Transcaruncular medial orbitotomy: A globe sparing intervention in management of COVID associated mucormycosis [CAM].Oman J Ophthalmol. 2023 Jun 27;16(2):268-275. doi: 10.4103/ojo.ojo_52_22. eCollection 2023 May-Aug. Oman J Ophthalmol. 2023. PMID: 37602165 Free PMC article.
-
Analysis of pathogenetic process of fungal rhinosinusitis: Report of two cases.World J Clin Cases. 2020 Jan 26;8(2):451-463. doi: 10.12998/wjcc.v8.i2.451. World J Clin Cases. 2020. PMID: 32047798 Free PMC article.
References
-
- Nicolai P., Lombardi D., Tomenzoli D. Fungus ball of the paranasal sinuses: experience in 160 patients treated with endoscopic surgery. Laryngoscope. 2009;119(11):2275–2279. - PubMed
-
- Hazarika P., Ravikumar V., Nayak R.G., Rao P.S., Shivananda P.G. Rhinocerebral mycosis. Ear Nose Throat J. 1984;63:464–468. - PubMed
-
- Bergstrom L., Hemenway W.G., Barnhart R.A. Rhinocerebral and otologic mucormycosis. Ann Otol Rhinol Laryngol. 1970;79:70–81. - PubMed
