

Treatment retention among patients randomized to buprenorphine/naloxone compared to methadone in a multi-site trial
- PMID: 23961726
- PMCID: PMC3947022
- DOI: 10.1111/add.12333
Treatment retention among patients randomized to buprenorphine/naloxone compared to methadone in a multi-site trial
Abstract
Aims: To examine patient and medication characteristics associated with retention and continued illicit opioid use in methadone (MET) versus buprenorphine/naloxone (BUP) treatment for opioid dependence.
Design, settings and participants: This secondary analysis included 1267 opioid-dependent individuals participating in nine opioid treatment programs between 2006 and 2009 and randomized to receive open-label BUP or MET for 24 weeks.
Measurements: The analyses included measures of patient characteristics at baseline (demographics; use of alcohol, cigarettes and illicit drugs; self-rated mental and physical health), medication dose and urine drug screens during treatment, and treatment completion and days in treatment during the 24-week trial.
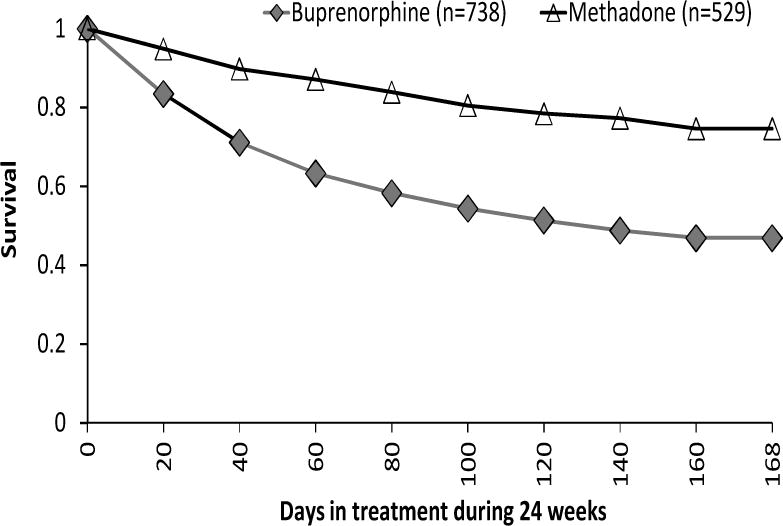
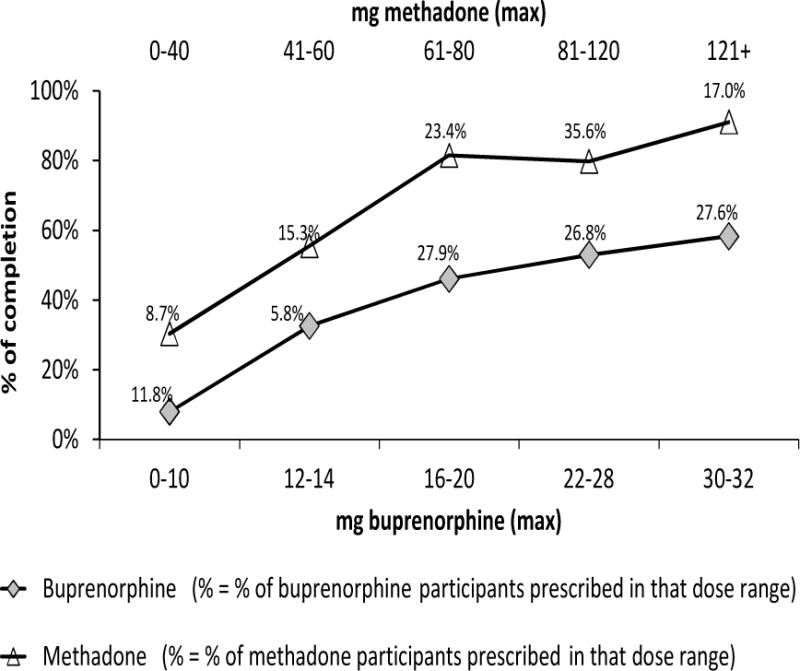
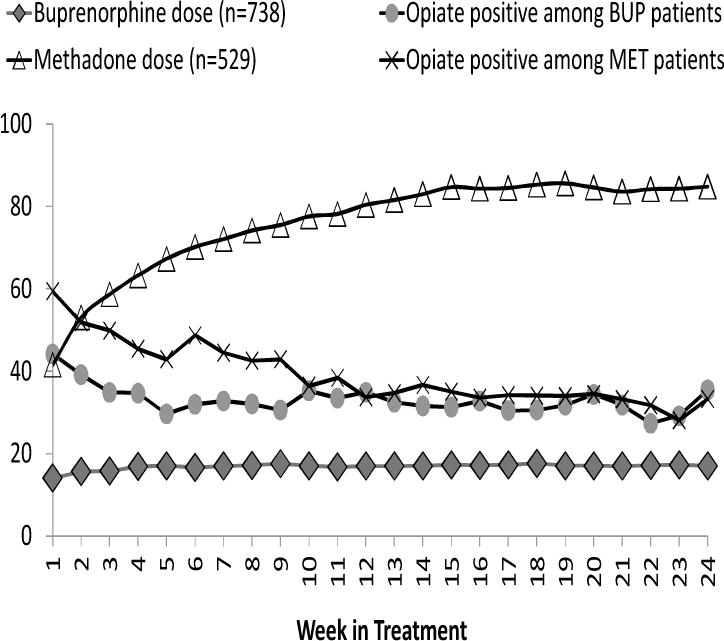
Findings: The treatment completion rate was 74% for MET versus 46% for BUP (P < 0.01); the rate among MET participants increased to 80% when the maximum MET dose reached or exceeded 60 mg/day. With BUP, the completion rate increased linearly with higher doses, reaching 60% with doses of 30-32 mg/day. Of those remaining in treatment, positive opioid urine results were significantly lower [odds ratio (OR) = 0.63, 95% confidence interval (CI) = 0.52-0.76, P < 0.01] among BUP relative to MET participants during the first 9 weeks of treatment. Higher medication dose was related to lower opiate use, more so among BUP patients. A Cox proportional hazards model revealed factors associated with dropout: (i) BUP [versus MET, hazard ratio (HR) = 1.61, CI = 1.20-2.15], (ii) lower medication dose (<16 mg for BUP, <60 mg for MET; HR = 3.09, CI = 2.19-4.37), (iii) the interaction of dose and treatment condition (those with higher BUP dose were 1.04 times more likely to drop out than those with lower MET dose, and (iv) being younger, Hispanic and using heroin or other substances during treatment.
Conclusions: Provision of methadone appears to be associated with better retention in treatment for opioid dependence than buprenorphine, as does use of provision of higher doses of both medications. Provision of buprenorphine is associated with lower continued use of illicit opioids.
Trial registration: ClinicalTrials.gov NCT00315341.
Keywords: Buprenorphine; methadone; opiate dependence; treatment outcomes.
© 2013 Society for the Study of Addiction.
Conflict of interest statement
Declaration of Interest: Authors disclosing relevant financial interests, activities, relationships, and affiliations are:
Yih-Ing Hser: Received a small educational grant from Reckitt Benckiser Pharmaceuticals to support a Summer Institute on Promoting Recovery within the Changing Health Service System.
Andrew Saxon: Consultant to Reckitt Benckiser Pharmaceuticals. Advisory board member for Alkermes, Inc.
Walter Ling: Consultant to Reckitt Benckiser Pharmaceuticals.
All other authors report no financial or other possible conflicts of interest.
Figures
Comment in
-
Commentary on Hser et al. (2014): to retain or not to retain-open questions in opioid maintenance therapy.Addiction. 2014 Jan;109(1):88-9. doi: 10.1111/add.12376. Addiction. 2014. PMID: 24438113 No abstract available.
References
-
- Substance Abuse and Mental Health Services Administration. Results from the 2010 National Survey on Drug Use and Health: Summary of National Findings. Rockville, MD: 2011.
-
- Degenhardt L, Hall W. Extent of illicit drug use and dependence, and their contribution to the global burden of disease. Lancet. 2012 Jan 7;379(9810):55–70. - PubMed
-
- Warner M, Chen LH, Makuc DM, Anderson RN, Miniño AM. Drug poisoning deaths in the United States, 1980–2008. Hyattsville, MD: National Center for Health Statistics; 2011.
-
- Connock M, Juarez-Garcia A, Jowett S, Frew E, Liu Z, Taylor RJ, Fry-Smith A, Day E, Lintzeris N, Roberts T, Burls A, Taylor RS. Methadone and buprenorphine for the management of opioid dependence: a systematic review and economic evaluation. Health Technol Assess. 2007;11(9):1–171. iii–iv. - PubMed
-
- Bell J, Trinh L, Butler B, Randall D, Rubin G. Comparing retention in treatment and mortality in people after initial entry to methadone and buprenorphine treatment. Addiction. 2009;104(7):1193–200. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
