

Using a standardized method for laparoscopic cholecystectomy to create a concept operation-specific checklist
- PMID: 23961737
- PMCID: PMC4008160
- DOI: 10.1111/hpb.12161
Using a standardized method for laparoscopic cholecystectomy to create a concept operation-specific checklist
Abstract
Objectives: Prevalences of bile duct injury (BDI) following laparoscopic cholecystectomy (LC) remain unacceptably high. There is no standardized method for performing an LC. This study aims to describe a standardized technique for LC that will allow for the development of a concept LC checklist, the use of which, it is hoped, will decrease the prevalence of BDI.
Methods: A standardized method for LC was developed based on previously published expert analysis supplemented by video error analysis of operations in which BDI occurred. Established checklist methodology was then used to construct an LC-specific concept checklist.
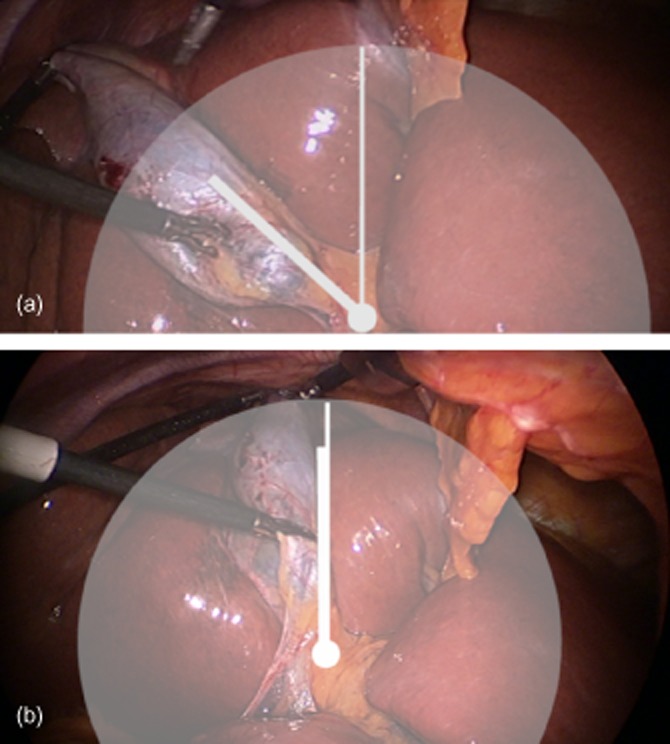
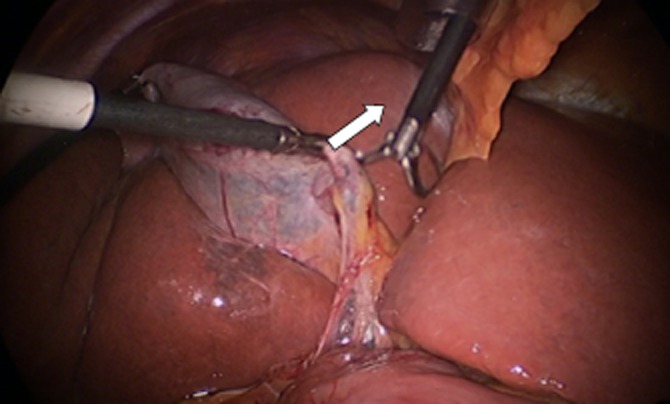
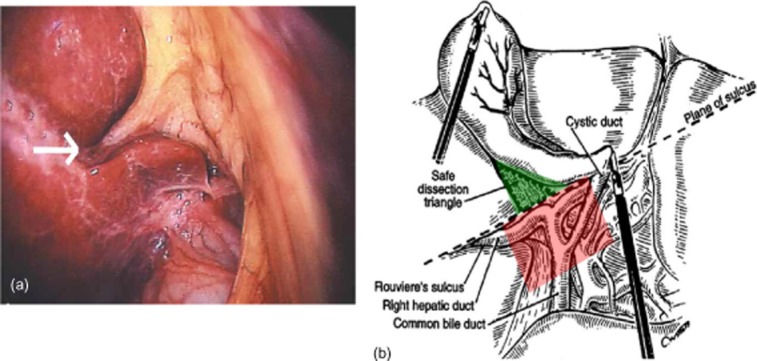
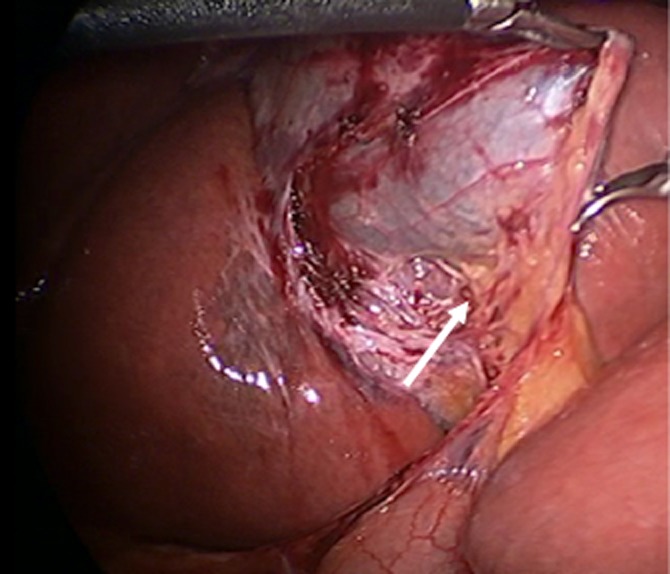
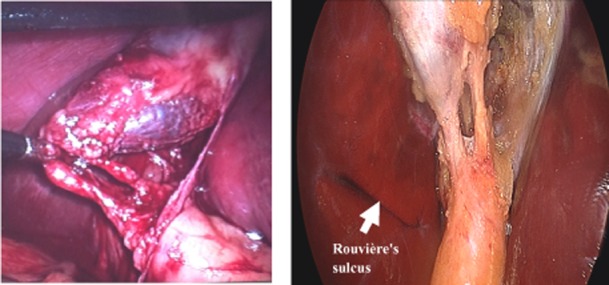
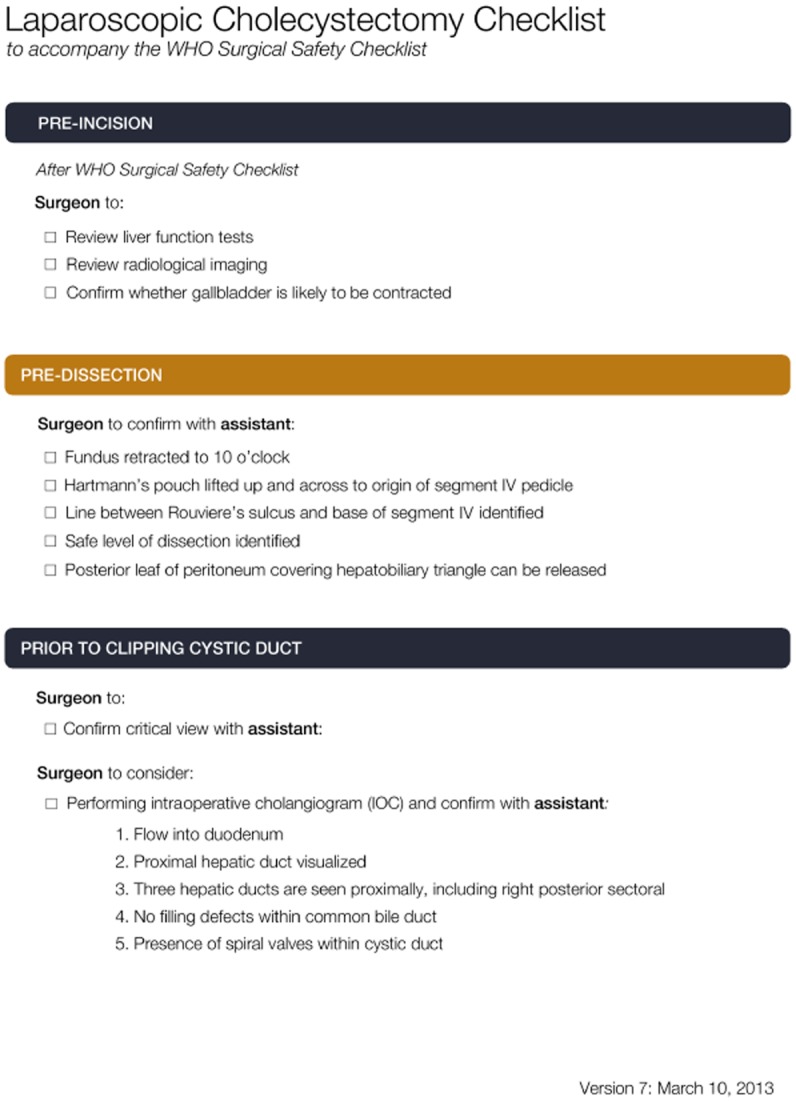
Results: A five-step technique for the safe establishment of the critical view was created to guide the development of the checklist. The five steps are: (i) confirm the gallbladder lies in the hepatic principal plane and is retracted to the 10 o'clock position; (ii) confirm Hartmann's pouch is lifted up and toward the segment IV pedicle; (iii) identify Rouvière's sulcus; (iv) confirm the release of the posterior leaf of the peritoneum covering the hepatobiliary triangle, and (v) confirm the critical view with or without intraoperative cholangiography.
Conclusions: A standardized approach to LC would allow for the creation of an LC-specific checklist that has the potential to lower the prevalence of BDI.
© 2013 International Hepato-Pancreato-Biliary Association.
Figures
Similar articles
-
Safe laparoscopic cholecystectomy: A systematic review of bile duct injury prevention.Int J Surg. 2018 Dec;60:164-172. doi: 10.1016/j.ijsu.2018.11.006. Epub 2018 Nov 12. Int J Surg. 2018. PMID: 30439536
-
A safe laparoscopic cholecystectomy depends upon the establishment of a critical view of safety.Surg Today. 2010 Jun;40(6):507-13. doi: 10.1007/s00595-009-4218-z. Epub 2010 May 23. Surg Today. 2010. PMID: 20496131
-
Iatrogenic bile duct injury: the scourge of laparoscopic cholecystectomy.ANZ J Surg. 2002 Feb;72(2):83-8. doi: 10.1046/j.1445-2197.2002.02315.x. ANZ J Surg. 2002. PMID: 12074081
-
A practical new strategy to prevent bile duct injury during laparoscopic cholecystectomy. A single-center experience with 5539 cases.Acta Cir Bras. 2020;35(6):e202000607. doi: 10.1590/s0102-865020200060000007. Epub 2020 Jul 8. Acta Cir Bras. 2020. PMID: 32667588 Free PMC article.
-
Tokyo Guidelines 2018: surgical management of acute cholecystitis: safe steps in laparoscopic cholecystectomy for acute cholecystitis (with videos).J Hepatobiliary Pancreat Sci. 2018 Jan;25(1):73-86. doi: 10.1002/jhbp.517. Epub 2018 Jan 10. J Hepatobiliary Pancreat Sci. 2018. PMID: 29095575 Review.
Cited by
-
Improving Safety in Laparoscopic Cholecystectomy: Reply.World J Surg. 2016 Jun;40(6):1536. doi: 10.1007/s00268-015-3350-8. World J Surg. 2016. PMID: 26608957 No abstract available.
-
Injuries during Laparoscopic Cholecystectomy: A Scoping Review of the Claims and Civil Action Judgements.J Clin Med. 2021 Nov 10;10(22):5238. doi: 10.3390/jcm10225238. J Clin Med. 2021. PMID: 34830520 Free PMC article.
-
Safe laparoscopic cholecystectomy: Adoption of universal culture of safety in cholecystectomy.World J Gastrointest Surg. 2019 Feb 27;11(2):62-84. doi: 10.4240/wjgs.v11.i2.62. World J Gastrointest Surg. 2019. PMID: 30842813 Free PMC article. Review.
-
An intraoperative artificial intelligence system identifying anatomical landmarks for laparoscopic cholecystectomy: a prospective clinical feasibility trial (J-SUMMIT-C-01).Surg Endosc. 2023 Mar;37(3):1933-1942. doi: 10.1007/s00464-022-09678-w. Epub 2022 Oct 19. Surg Endosc. 2023. PMID: 36261644 Clinical Trial.
-
Harmonic Scalpel Versus Clips for Ligation of Cystic Duct in Laparoscopic Cholecystectomy: A Systematic Review.Cureus. 2022 Dec 8;14(12):e32335. doi: 10.7759/cureus.32335. eCollection 2022 Dec. Cureus. 2022. PMID: 36505958 Free PMC article. Review.
References
-
- Russell JC, Walsh SJ, Mattie AS, Lynch JT. Bile duct injuries, 1989–1993. A state-wide experience. Connecticut Laparoscopic Cholecystectomy Registry. Arch Surg. 1996;131:382–388. - PubMed
-
- Richardson MC, Bell G, Fullarton GM. Incidence and nature of bile duct injuries following laparoscopic cholecystectomy: an audit of 5913 cases. West of Scotland Laparoscopic Cholecystectomy Audit Group. Br J Surg. 1996;83:1356–1360. - PubMed
-
- Flum DR, Dellinger EP, Cheadle A, Chan L, Koepsell T. Intraoperative cholangiography and risk of common bile duct injury during cholecystectomy. JAMA. 2003;289:1639–1644. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
