

Trials to improve blood pressure through adherence to antihypertensives in stroke/TIA: systematic review and meta-analysis
- PMID: 23963756
- PMCID: PMC3828799
- DOI: 10.1161/JAHA.113.000251
Trials to improve blood pressure through adherence to antihypertensives in stroke/TIA: systematic review and meta-analysis
Abstract
Background: The purpose of this study was to determine whether interventions including components to improve adherence to antihypertensive medications in patients after stroke/transient ischemic attack (TIA) improve adherence and blood pressure control.
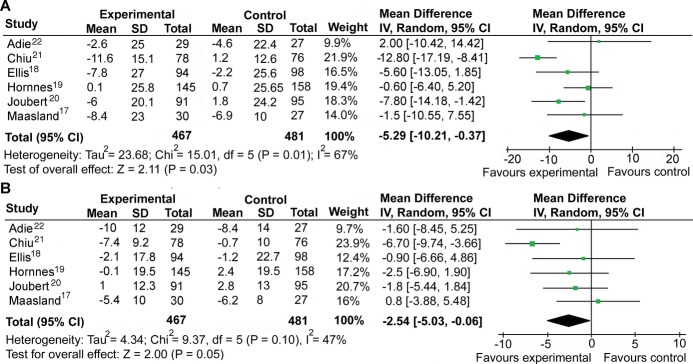
Methods and results: We searched MEDLINE, EMBASE, CINAHL, BNI, PsycINFO, and article reference lists to October 2012. Search terms included stroke/TIA, adherence/prevention, hypertension, and randomized controlled trial (RCT). Inclusion criteria were participants with stroke/TIA; interventions including a component to improve adherence to antihypertensive medications; and outcomes including blood pressure, antihypertensive adherence, or both. Two reviewers independently assessed studies to determine eligibility, validity, and quality. Seven RCTs were eligible (n=1591). Methodological quality varied. All trials tested multifactorial interventions. None targeted medication adherence alone. Six trials measured blood pressure and 3 adherence. Meta-analysis of 6 trials showed that multifactorial programs were associated with improved blood pressure control. The difference between intervention versus control in mean improvement in systolic blood pressure was -5.3 mm Hg (95% CI, -10.2 to -0.4 mm Hg, P=0.035; I(2)=67% [21% to 86%]) and in diastolic blood pressure was -2.5 mm Hg (-5.0 to -0.1 mm Hg, P=0.046; I(2)=47% [0% to 79%]). There was no effect on medication adherence where measured.
Conclusions: Multifactorial interventions including a component to improve medication adherence can lower blood pressure after stroke/TIA. However, it is not possible to say whether or not this is achieved through better medication adherence. Trials are needed of well-characterized interventions to improve medication adherence and clinical outcomes with measurement along the hypothesized causal pathway.
Keywords: blood pressure; hypertension; prevention; stroke.
Figures



Similar articles
-
Antihypertensive withdrawal for the prevention of cognitive decline.Cochrane Database Syst Rev. 2016 Nov 1;11(11):CD011971. doi: 10.1002/14651858.CD011971.pub2. Cochrane Database Syst Rev. 2016. PMID: 27802359 Free PMC article.
-
Interventions for improving modifiable risk factor control in the secondary prevention of stroke.Cochrane Database Syst Rev. 2018 May 7;5(5):CD009103. doi: 10.1002/14651858.CD009103.pub3. Cochrane Database Syst Rev. 2018. PMID: 29734470 Free PMC article.
-
Mobile phone-based interventions for improving adherence to medication prescribed for the primary prevention of cardiovascular disease in adults.Cochrane Database Syst Rev. 2018 Jun 22;6(6):CD012675. doi: 10.1002/14651858.CD012675.pub2. Cochrane Database Syst Rev. 2018. Update in: Cochrane Database Syst Rev. 2021 Mar 26;3:CD012675. doi: 10.1002/14651858.CD012675.pub3. PMID: 29932455 Free PMC article. Updated.
-
Mobile phone text messaging for medication adherence in secondary prevention of cardiovascular disease.Cochrane Database Syst Rev. 2024 Mar 27;3(3):CD011851. doi: 10.1002/14651858.CD011851.pub3. Cochrane Database Syst Rev. 2024. PMID: 38533994 Free PMC article.
-
Withdrawal of antihypertensive drugs in older people.Cochrane Database Syst Rev. 2025 Mar 31;3(3):CD012572. doi: 10.1002/14651858.CD012572.pub3. Cochrane Database Syst Rev. 2025. PMID: 40162571
Cited by
-
Are home visits an effective method for diabetes management? A quantitative systematic review and meta-analysis.J Diabetes Investig. 2017 Sep;8(5):701-708. doi: 10.1111/jdi.12630. Epub 2017 Mar 11. J Diabetes Investig. 2017. PMID: 28109182 Free PMC article.
-
Task shifting interventions for cardiovascular risk reduction in low-income and middle-income countries: a systematic review of randomised controlled trials.BMJ Open. 2014 Oct 16;4(10):e005983. doi: 10.1136/bmjopen-2014-005983. BMJ Open. 2014. PMID: 25324324 Free PMC article.
-
The Autonomic Regulation of Circulation and Adverse Events in Hypertensive Patients during Follow-Up Study.Cardiol Res Pract. 2019 Dec 30;2019:8391924. doi: 10.1155/2019/8391924. eCollection 2019. Cardiol Res Pract. 2019. PMID: 32082622 Free PMC article.
-
Adherence to medication in stroke survivors dependent on caregivers.Br J Gen Pract. 2015 Nov;65(640):e789-91. doi: 10.3399/bjgp15X687589. Br J Gen Pract. 2015. PMID: 26500329 Free PMC article. No abstract available.
-
What is the quantity, quality and type of systematic review evidence available to inform the optimal prescribing of statins and antihypertensives? A systematic umbrella review and evidence and gap map.BMJ Open. 2024 Feb 24;14(2):e072502. doi: 10.1136/bmjopen-2023-072502. BMJ Open. 2024. PMID: 38401904 Free PMC article.
References
-
- World Health Organization Preventing Chronic Disease: A Vital Investment. 2005Geneva: World Health Organization
-
- Arima H, Tzourio C, Butcher K, Anderson C, Bousser MG, Lees KR, Reid JL, Omae T, Woodward M, MacMahon S, Chalmers JPROGRESS Collaborative Group Prior events predict cerebrovascular and coronary outcomes in the PROGRESS trial. Stroke. 2006; 37:1497-1502 - PubMed
-
- Hankey G, Jamrozik K, Broadhurst R, Forbes S, Burvill PW, Anderson CS, Stewart‐Wynne EG. Long‐term risk of first recurrent stroke in the Perth Community Stroke Study. Stroke. 1998; 29:2491-2500 - PubMed
-
- Mant J, Wade DT, Winner S. In: Stevens A, Raftery J, Mant J, Simpson S. (eds.). Health care needs assessment: stroke. Health Care Needs Assessment: The Epidemiologically Based Needs Assessment Reviews, First Series. 20042nd edOxford: Radcliffe Medical Press; 141-244
-
- Jørgensen HS, Nakayama H, Reith J, Raaschou HO, Olsen TS. Stroke recurrence: predictors, severity, and prognosis. The Copenhagen Stroke Study. Neurology. 1997; 48:891-895 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
