

Myocardial tissue remodeling in adolescent obesity
- PMID: 23963758
- PMCID: PMC3828806
- DOI: 10.1161/JAHA.113.000279
Myocardial tissue remodeling in adolescent obesity
Abstract
Background: Childhood obesity is a significant risk factor for cardiovascular disease in adulthood. Although ventricular remodeling has been reported in obese youth, early tissue-level markers within the myocardium that precede organ-level alterations have not been described.
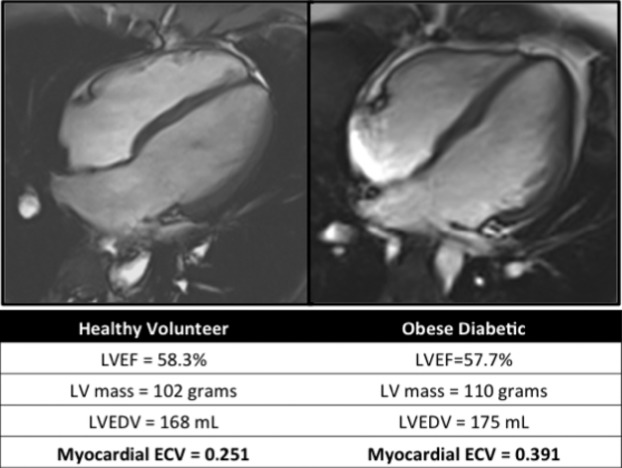
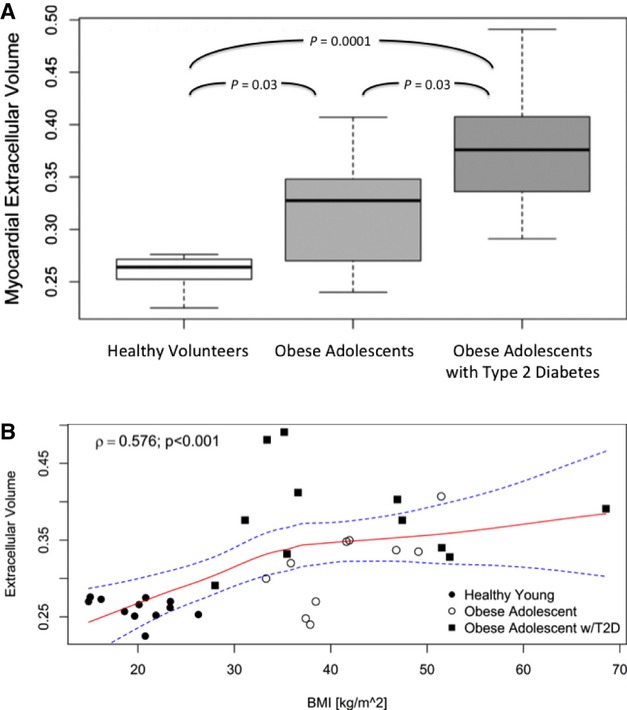
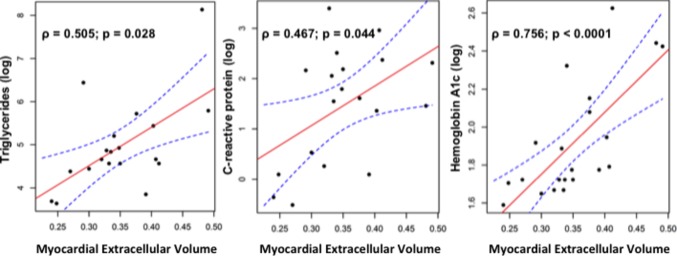
Methods and results: We studied 21 obese adolescents (mean age, 17.7±2.6 years; mean body mass index [BMI], 41.9±9.5 kg/m(2), including 11 patients with type 2 diabetes [T2D]) and 12 healthy volunteers (age, 15.1±4.5 years; BMI, 20.1±3.5 kg/m(2)) using biomarkers of cardiometabolic risk and cardiac magnetic resonance imaging (CMR) to phenotype cardiac structure, function, and interstitial matrix remodeling by standard techniques. Although left ventricular ejection fraction and left atrial volumes were similar in healthy volunteers and obese patients (and within normal body size-adjusted limits), interstitial matrix expansion by CMR extracellular volume fraction (ECV) was significantly different between healthy volunteers (median, 0.264; interquartile range [IQR], 0.253 to 0.271), obese adolescents without T2D (median, 0.328; IQR, 0.278 to 0.345), and obese adolescents with T2D (median, 0.376; IQR, 0.336 to 0.407; P=0.0001). ECV was associated with BMI for the entire population (r=0.58, P<0.001) and with high-sensitivity C-reactive protein (r=0.47, P<0.05), serum triglycerides (r=0.51, P<0.05), and hemoglobin A1c (r=0.76, P<0.0001) in the obese stratum.
Conclusions: Obese adolescents (particularly those with T2D) have subclinical alterations in myocardial tissue architecture associated with inflammation and insulin resistance. These alterations precede significant left ventricular hypertrophy or decreased cardiac function.
Keywords: CT or MRI; obesity; type 2 diabetes.
Figures
References
-
- Ogden CL, Carroll MD, Curtin LR, McDowell MA, Tabak CJ, Flegal KM. Prevalence of overweight and obesity in the United States, 1999–2004. JAMA. 2006; 295:1549-1555 - PubMed
-
- Steinberger J, Moran A, Hong CP, Jacobs DR, Jr, Sinaiko AR. Adiposity in childhood predicts obesity and insulin resistance in young adulthood. J Pediatr. 2001; 138:469-473 - PubMed
-
- Reilly JJ, Kelly J. Long‐term impact of overweight and obesity in childhood and adolescence on morbidity and premature mortality in adulthood: systematic review. Int J Obes (Lond). 2011; 35:891-898 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
