

Vasculopathy, inflammation, and blood flow in leg ulcers of patients with sickle cell anemia
- PMID: 23963836
- PMCID: PMC3946883
- DOI: 10.1002/ajh.23571
Vasculopathy, inflammation, and blood flow in leg ulcers of patients with sickle cell anemia
Abstract
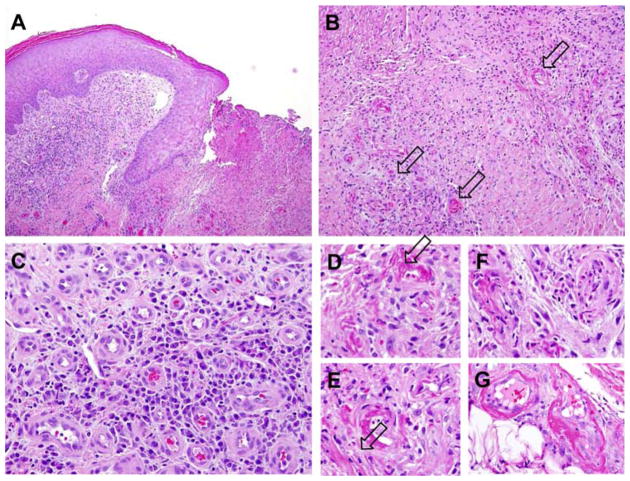
Chronic leg ulcers are frequent and debilitating complications of sickle cell anemia. Inadequate blood supply has been postulated to be an important factor in their occurrence and delayed healing. Little is known about their microcirculatory and histopathological changes. We evaluated the microcirculation of lower extremity ulcers with laser speckle contrast imaging and infrared thermography and obtained clinical and laboratory characteristics in 18 adults with sickle cell anemia and chronic leg ulcers. Skin biopsies were obtained in four subjects. Subjects had markers of severe disease, anemia, high degree of hemolysis, inflammation, and thrombophilia. The highest blood flow was present in the ulcer bed, progressively less in the immediate periwound area, and an unaffected control skin area in the same extremity. Microscopic examination showed evidence of venostasis, inflammation, and vasculopathy. Blood vessels were increased in number, had activated endothelium and evidence of thrombosis/recanalization. High blood flow may be due to chronic inflammation, cutaneous vasodilatation, venostasis, and in situ thrombosis. These changes in skin microcirculation are similar to chronic venous ulcers in the non-sickle cell disease (SCD) population, thus suggesting that leg ulcers may be another end-organ complication with endothelial dysfunction that appears in patients with SCD at a younger age and with higher frequency than in the general population.
Copyright © 2013 Wiley Periodicals, Inc.
Figures

References
-
- Eckman JR. Leg ulcers in sickle cell disease. Hematol Oncol Clin North Am. 1996;10:1333–1344. - PubMed
-
- Borgna-Pignatti C, Marsella M, Zanforlin N. The natural history of thalassemia intermedia. Ann N Y Acad Sci. 2010;1202:214–220. - PubMed
-
- Giraldi S, Abbage KT, Marinoni LP, et al. Leg ulcer in hereditary spherocytosis. Pediatr Dermatol. 2003;20:427–428. - PubMed
-
- Parent F, Bachir D, Inamo J, et al. A hemodynamic study of pulmonary hypertension in sickle cell disease. N Engl J Med. 2011;365:44–53. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical