

Regional health care planning: a methodology to cluster facilities using community utilization patterns
- PMID: 23964905
- PMCID: PMC3766152
- DOI: 10.1186/1472-6963-13-333
Regional health care planning: a methodology to cluster facilities using community utilization patterns
Abstract
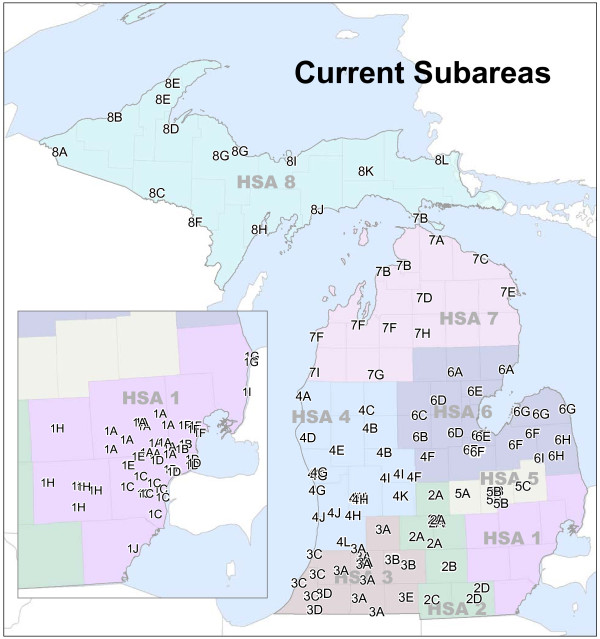
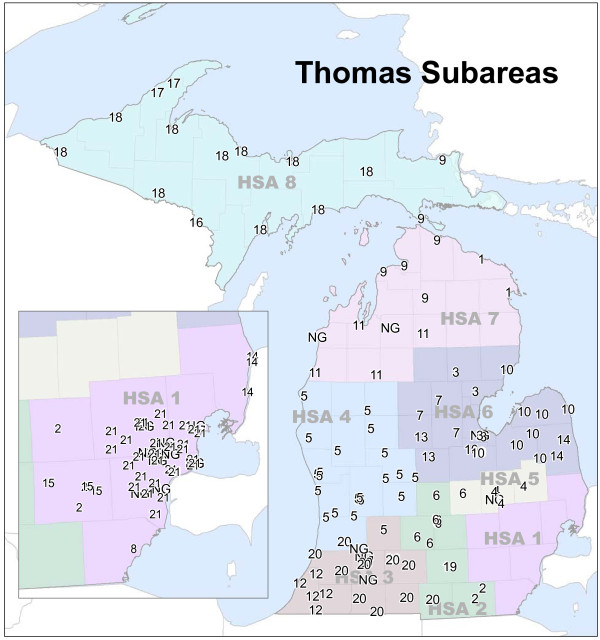
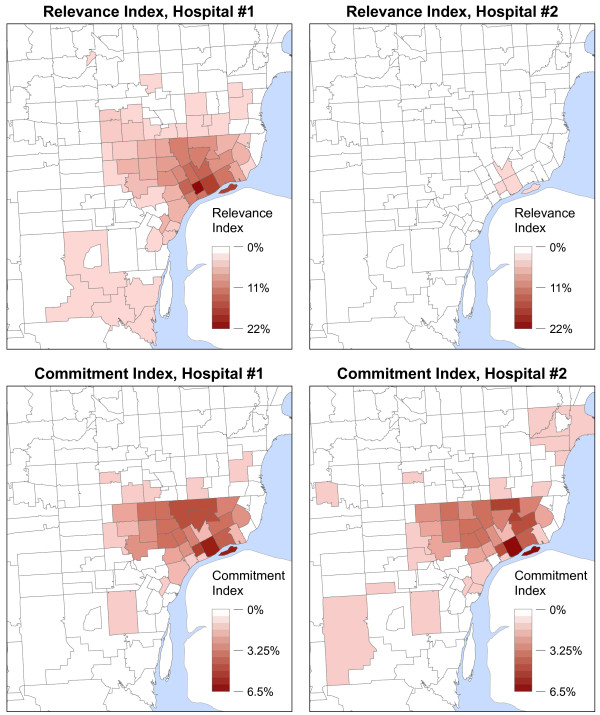
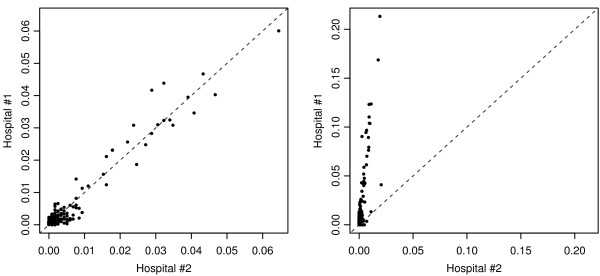
Background: Community-based health care planning and regulation necessitates grouping facilities and areal units into regions of similar health care use. Limited research has explored the methodologies used in creating these regions. We offer a new methodology that clusters facilities based on similarities in patient utilization patterns and geographic location. Our case study focused on Hospital Groups in Michigan, the allocation units used for predicting future inpatient hospital bed demand in the state's Bed Need Methodology. The scientific, practical, and political concerns that were considered throughout the formulation and development of the methodology are detailed.
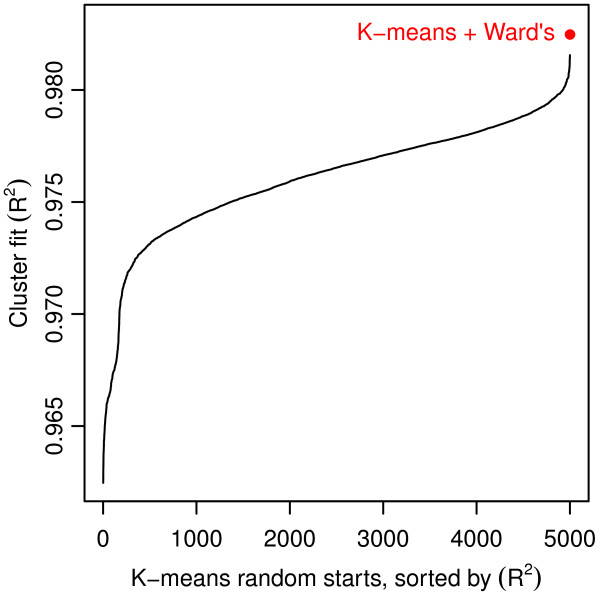
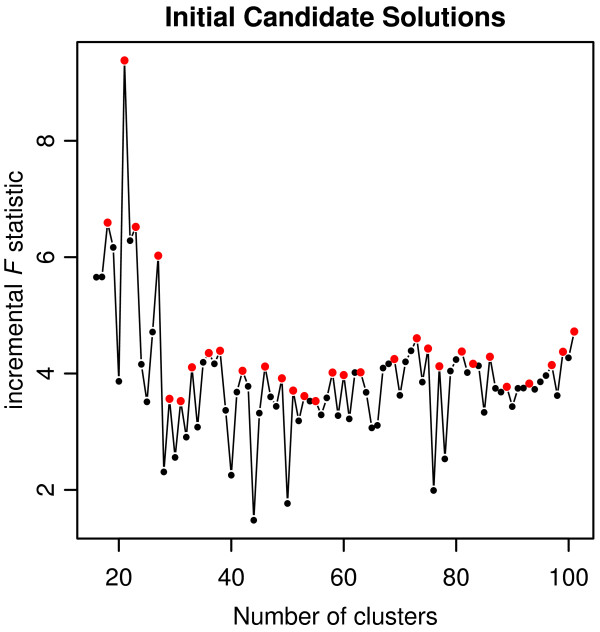
Methods: The clustering methodology employs a 2-step K-means + Ward's clustering algorithm to group hospitals. The final number of clusters is selected using a heuristic that integrates both a statistical-based measure of cluster fit and characteristics of the resulting Hospital Groups.
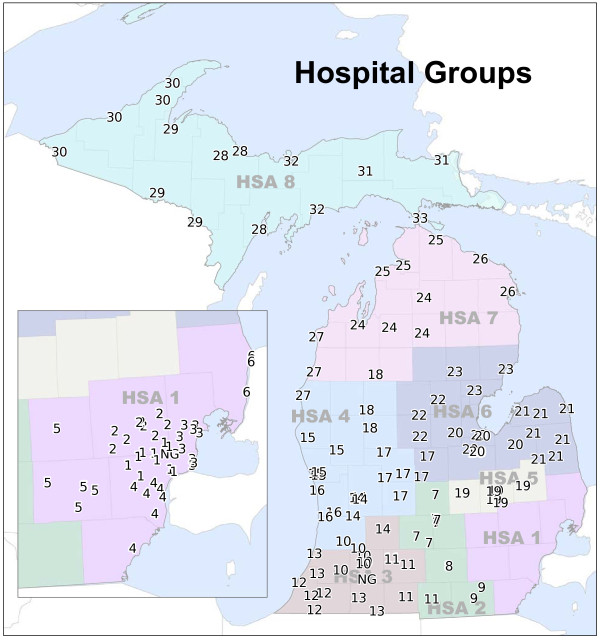
Results: Using recent hospital utilization data, the clustering methodology identified 33 Hospital Groups in Michigan.
Conclusions: Despite being developed within the politically charged climate of Certificate of Need regulation, we have provided an objective, replicable, and sustainable methodology to create Hospital Groups. Because the methodology is built upon theoretically sound principles of clustering analysis and health care service utilization, it is highly transferable across applications and suitable for grouping facilities or areal units.
Figures
References
-
- US Federal Trade Commission and US Department of Justice. Improving Health Care: A Dose of Competition. Washington, D.C: Tech. rep., US, Government Printing Office; 2004.
-
- Rivers PA, Fottler MD, Younis MZ. Does certificate of need really contain hospital costs in the United States? Health Edu J. 2007;66(3):229–244. doi: 10.1177/0017896907080127. - DOI
-
- National Conference of State Legislatures. CON-certificate of need state laws. 2011. [ http://www.ncsl.org/issues-research/health/con-certificate-of-need-state...]
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
