

Levels and changes of HDL cholesterol and apolipoprotein A-I in relation to risk of cardiovascular events among statin-treated patients: a meta-analysis
- PMID: 23965489
- PMCID: PMC3807966
- DOI: 10.1161/CIRCULATIONAHA.113.002670
Levels and changes of HDL cholesterol and apolipoprotein A-I in relation to risk of cardiovascular events among statin-treated patients: a meta-analysis
Abstract
Background: It is unclear whether levels of high-density lipoprotein cholesterol (HDL-C) or apolipoprotein A-I (apoA-I) remain inversely associated with cardiovascular risk among patients who achieve very low levels of low-density lipoprotein cholesterol on statin therapy. It is also unknown whether a rise in HDL-C or apoA-I after initiation of statin therapy is associated with a reduced cardiovascular risk.
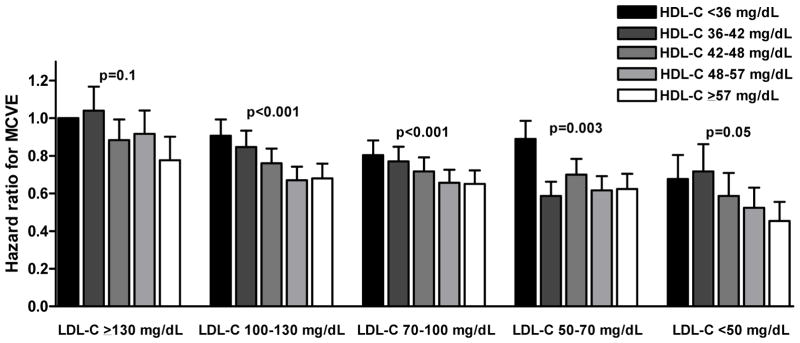
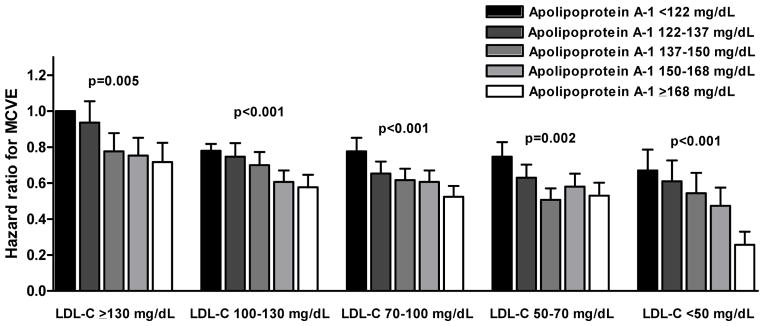
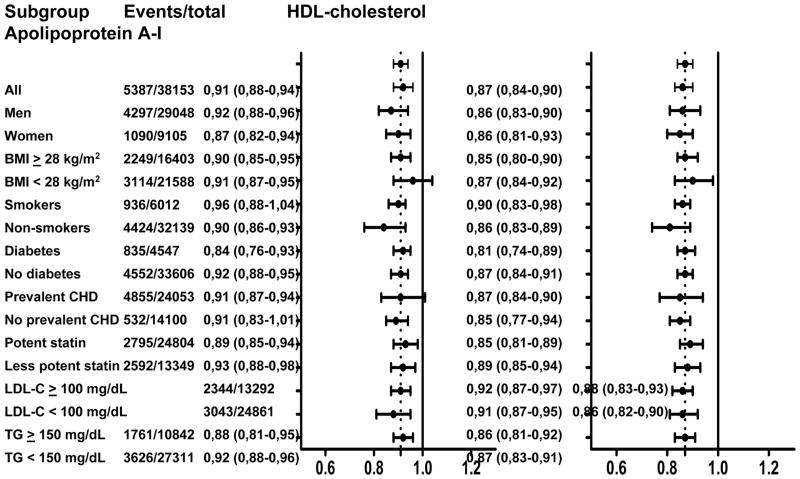
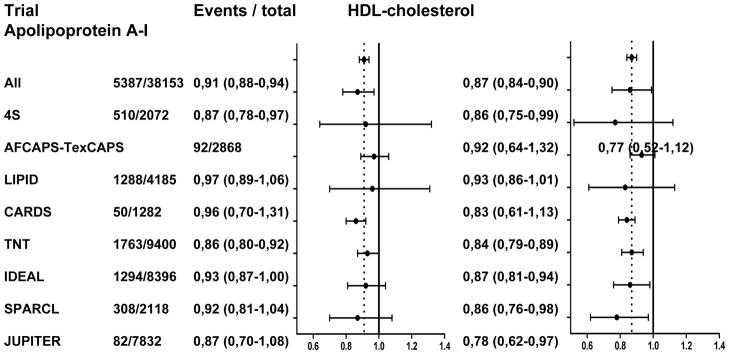
Methods and results: We performed a meta-analysis of 8 statin trials in which lipids and apolipoproteins were determined in all study participants at baseline and at 1-year follow-up. Individual patient data were obtained for 38,153 trial participants allocated to statin therapy, of whom 5387 suffered a major cardiovascular event. HDL-C levels were associated with a reduced risk of major cardiovascular events (adjusted hazard ratio [HR], 0.83; 95% confidence interval [CI], 0.81-0.86 per 1 standard deviation increment), as were apoA-I levels (HR, 0.79; 95% CI, 0.72-0.82). This association was also observed among patients achieving on-statin low-density lipoprotein cholesterol levels <50 mg/dL. An increase of HDL-C was not associated with reduced cardiovascular risk (HR, 0.98; 95% CI, 0.94-1.01 per 1 standard deviation increment), whereas a rise in apoA-I was (HR, 0.93; 95% CI, 0.90-0.97).
Conclusions: Among patients treated with statin therapy, HDL-C and apoA-I levels were strongly associated with a reduced cardiovascular risk, even among those achieving very low low-density lipoprotein cholesterol. An apoA-I increase was associated with a reduced risk of major cardiovascular events, whereas for HDL-C this was not the case. These findings suggest that therapies that increase apoA-I concentration require further exploration with regard to cardiovascular risk reduction.
Keywords: apolipoproteins; cardiovascular diseases; high-density lipoprotein cholesterol; meta-analysis.
Conflict of interest statement
Drs Boekholdt, Arsenault and Hovingh report receipt of consultancy fees from Pfizer. Dr Mora reports receipt of research grant support through her institution from Merck Sharpe & Dohme and AstraZeneca; consultancy fees from Pfizer and Quest Diagnostics; lecture honoraria from AstraZeneca and Abbott; and travel accommodations/meeting expenses from Pfizer. Dr LaRosa reports receipt of consultancy fees from Pfizer and Amgen, and travel expenses from Pfizer. Dr Pedersen reports receipt of research grant support and lecture fees from Pfizer and Merck Sharp & Dohme and lecture fees from AstraZeneca and Roche. Dr DeMicco reports being a full-time employee of Pfizer; and having stock/stock options with Pfizer. Dr Welch reports receipt of a grant, consulting fees, travel support, payment for writing or manuscript review, and provision of writing assistance, medicines, equipment, or administrative support from Pfizer, and provision of consultancy services to Edwards, MAP, and NuPathe. Dr Amarenco reports receipt of research grant support and lecture fees from Pfizer, Sanofi, Merck, AstraZeneca, Boehringer-Ingelheim, and consultancy fees from Pfizer, BMS, Merck, Boehringer-Ingelheim, AstraZeneca, Bayer, Daiichi-Sankyo, Lundbeck, Edwards, Boston Scientific, Kowa and research grants from the French government. Dr Tonkin reports receipt of consultancy fees from Amgen, AstraZeneca, Boehringer-Ingelheim, Merck Sharpe & Dohme, Pfizer and Regeneron; and lecture honoraria from AstraZeneca, Merck Sharpe & Dohme, and Roche. Dr Colhoun reports receipt of research grant support through the EU Innovative Medicines Initiative from Roche, Pfizer, Eli Lilly, Boehringer-Ingelheim, and AstraZeneca; consultancy fees from Pfizer, sanofi-aventis, Novartis, and Eli Lilly; and lecture honoraria and travel expenses from Pfizer. Dr Betteridge reports receipt of honoraria for lectures and advisory boards for Aegerion, Amgen, AstraZeneca, Kowa, Merck Sharpe & Dohme, Roche, and Takeda. Dr Hitman has received consultancy fees and lecture honoraria from GlaxoSmithKline, Eli Lily, Pfizer, NovoNordisk, Astra Zeneca, Merck Sharp & Dohme, Takeda and OSI Pharmaceuticals and grant income from Park Davies and Eli Lily. Dr Gotto is a consultant for AstraZeneca, Janssen, KOWA, Merck, and Roche; a member of the Board of Directors for Aegerion Pharmaceuticals and Arisaph Pharmaceuticals; and a member of advisory boards for DuPont, Haptocure, VascuVis, and VateraCapital. Dr Clearfield reports provision of consulting services on advisory committees to Merck Sharp & Dohme and AstraZeneca. Dr Ridker reports receipt of research grant funding from Novartis and AstraZeneca; serving as a consultant to ISIS, Vascular Biogenics, Merck Sharpe & Dohme, Abbott, and Boehringer-Ingelheim; board membership with Merck Sharp & Dohme; receipt of a grant or pending grant to his institution from Amgen; and being listed as a coinventor on patents held by the Brigham and Women’s Hospital that relate to the use of inflammatory biomarkers in cardiovascular disease and diabetes that have been licensed to AstraZeneca and Siemens. Dr Kastelein reports receipt of lecture honoraria from Merck Sharpe & Dohme, Roche, Novartis, ISIS, Genzyme, Pfizer, Kowa, and AstraZeneca. Drs Downs, Durrington, Kirby and Sullivan reported no conflict of interest.
Figures
References
-
- Wilson PW, Garrison RJ, Castelli WP, et al. Prevalence of coronary heart disease in the Framingham Offspring Study: role of lipoprotein cholesterols. Am J Cardiol. 1980;46:649–654. - PubMed
-
- deGoma EM, Leeper NJ, Heidenreich PA. Clinical significance of high-density lipoprotein cholesterol in patients with low low-density lipoprotein cholesterol. J Am Coll Cardiol. 2008;51:49–55. - PubMed
-
- Sacks FM, Tonkin AM, Shepherd J, et al. Effect of pravastatin on coronary disease events in subgroups defined by coronary risk factors: the Prospective Pravastatin Pooling Project. Circulation. 2000;102:1893–1900. - PubMed
-
- Barter P, Gotto AM, LaRosa JC, et al. HDL cholesterol, very low levels of LDL cholesterol, and cardiovascular events. N Engl J Med. 2007;357:1301–1310. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
