

Sulfonylurea receptor 1 expression in human cerebral infarcts
- PMID: 23965746
- PMCID: PMC3771575
- DOI: 10.1097/NEN.0b013e3182a32e40
Sulfonylurea receptor 1 expression in human cerebral infarcts
Abstract
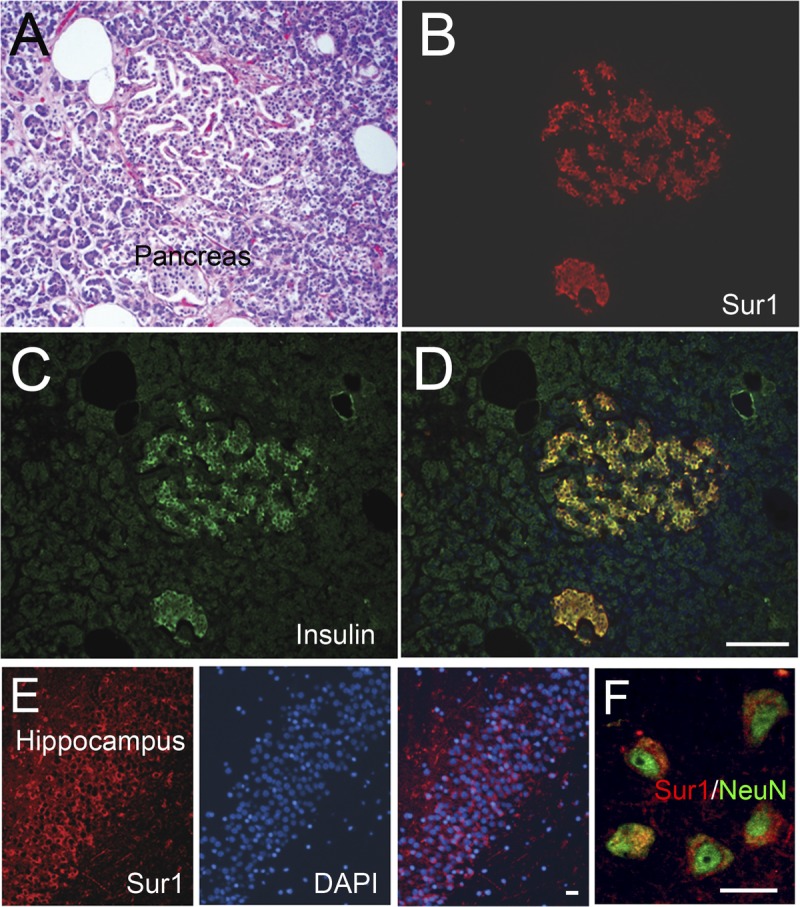
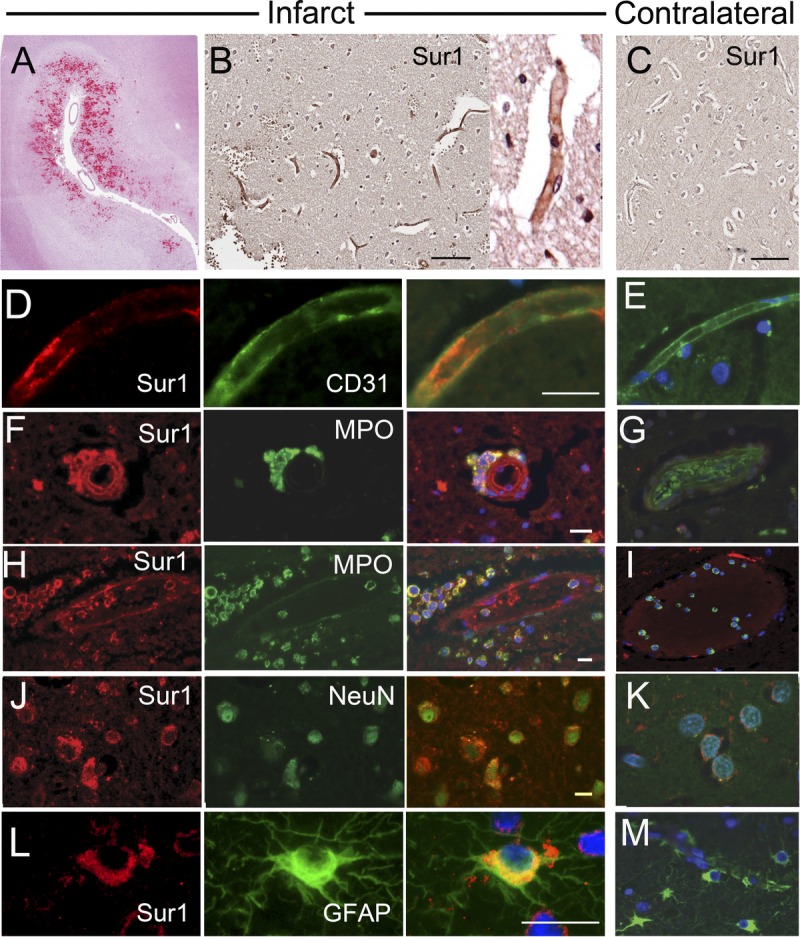
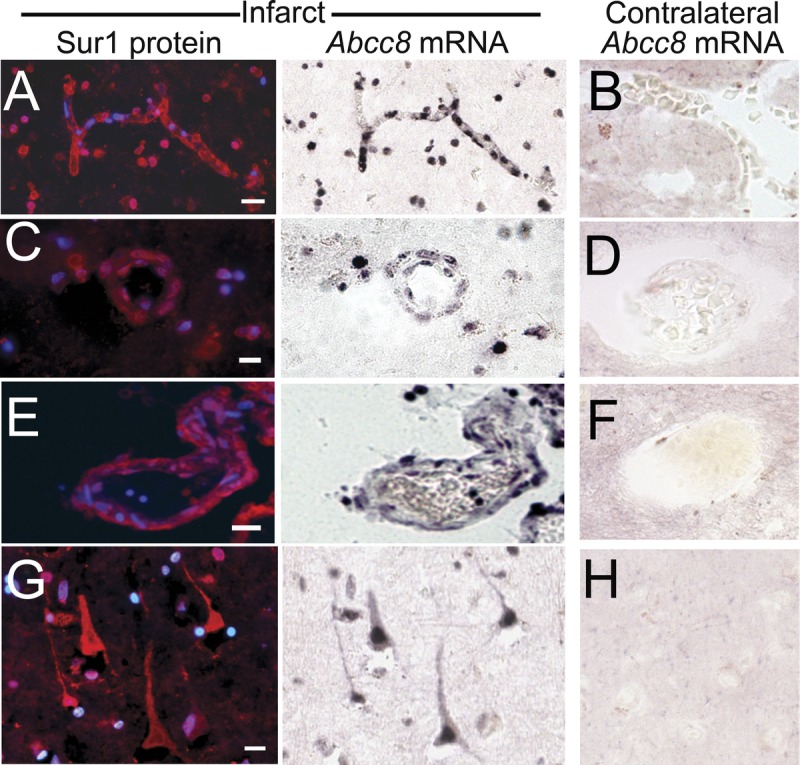
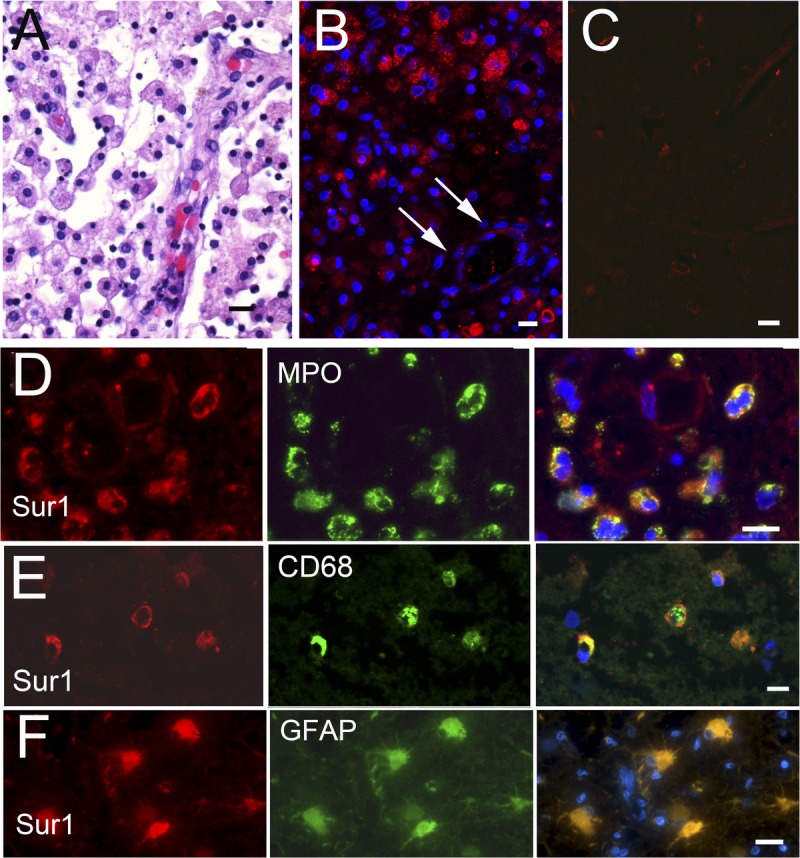
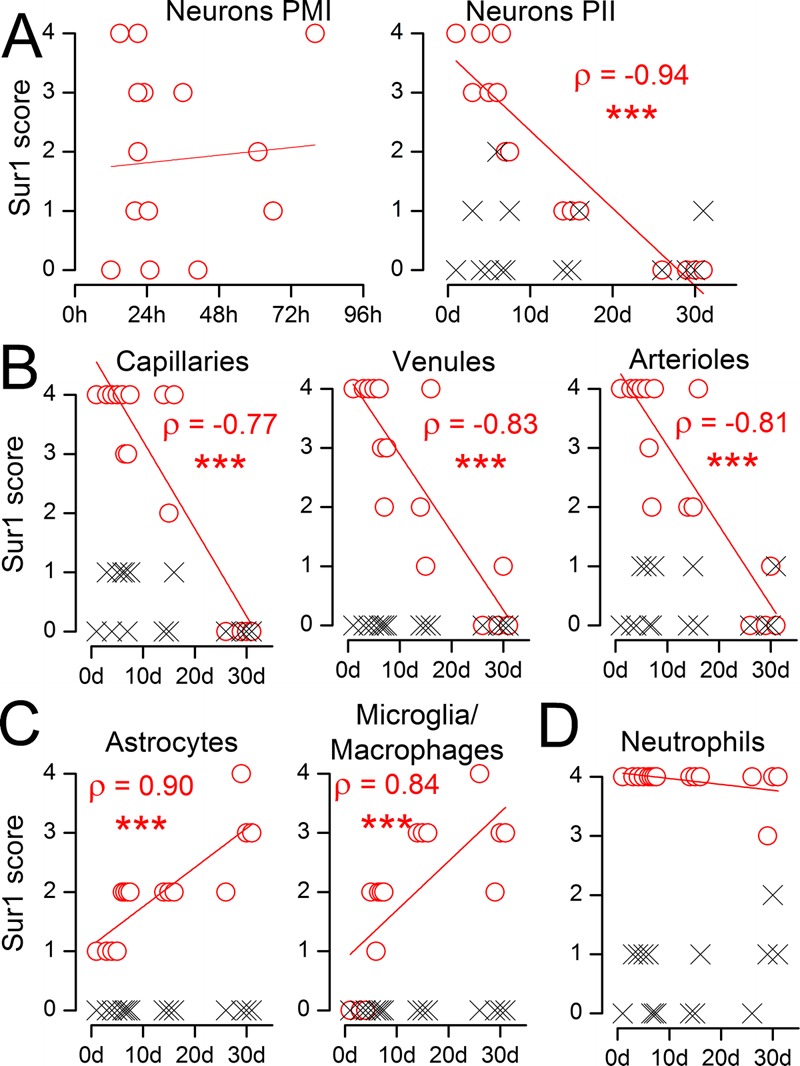
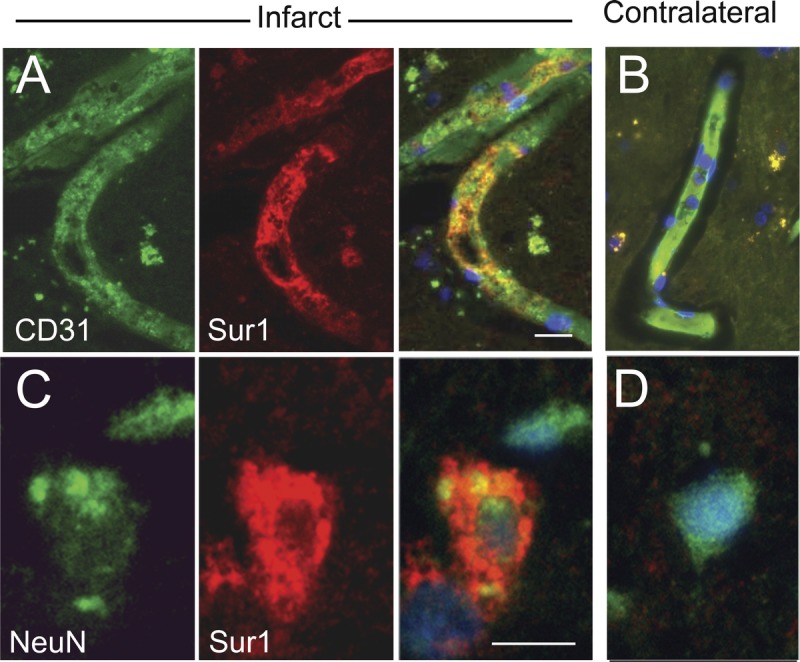
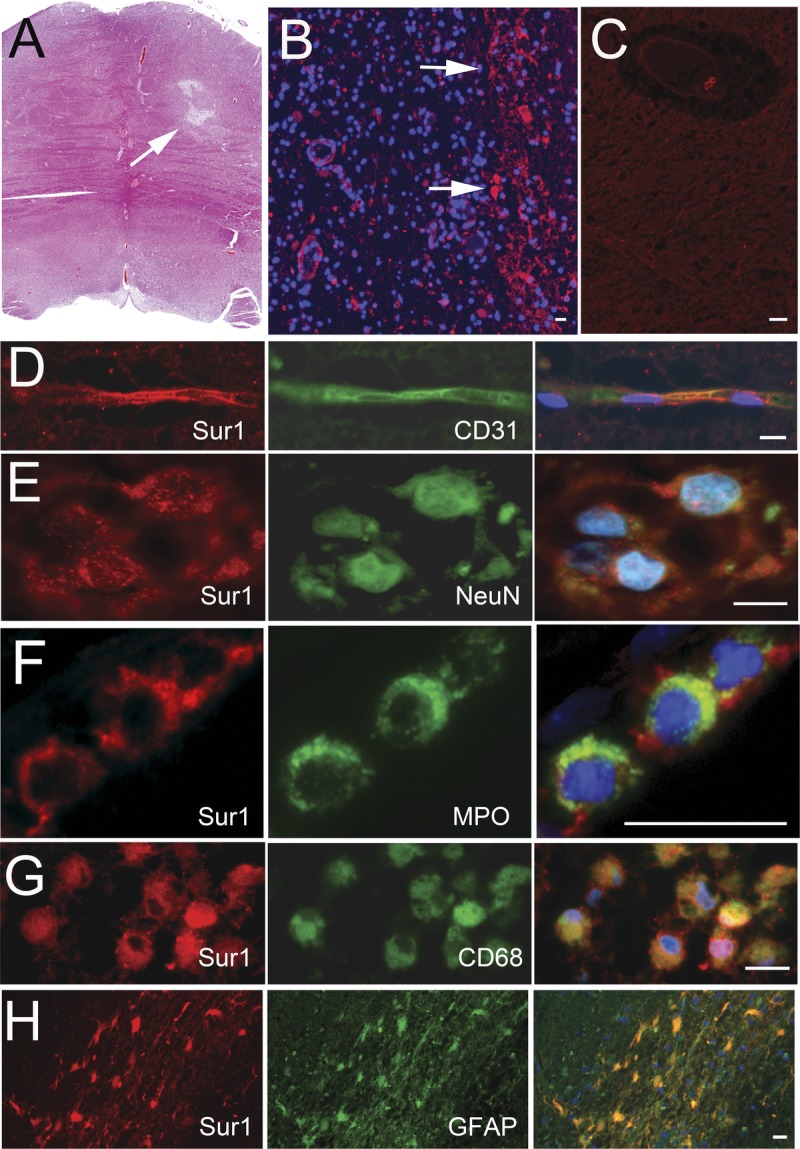
In animal models of stroke, sulfonylurea receptor 1 (Sur1), a member of the adenosine triphosphate binding cassette transporter gene family, is transcriptionally upregulated in neural and vascular cells in which it plays a leading role in edema formation and necrotic cell death. To date, expression of Sur1 in the brains of humans with cerebral infarcts has not been systematically evaluated. We examined Sur1 expression in postmortem specimens obtained from 13 patients within the first 31 days after focal infarcts, 5 patients with lacunar infarcts, and 6 normal control brains using immunohistochemistry. Elevated immunoreactivity for Sur1 was detected in all cases of focal infarcts, with 3 distinct temporal patterns of expression: 1) neurons and endothelium showed the greatest elevation during the first week, after which levels declined; 2) astrocytes and microglia/macrophages showed progressive increases during the first 31 days; and 3) neutrophils near the infarct showed prominent immunoreactivity that did not change over time. Upregulation of Sur1 was corroborated using in situ hybridization for Abcc8 mRNA. Sulfonylurea receptor 1 immunoreactivity in lacunar infarcts was less prominent and more sporadic than in nonlacunar infarcts. In conjunction with previous studies, these data suggest that Sur1 may be a promising treatment target in patients with acute cerebral infarction.
Figures
References
-
- Truelsen T, Begg S, Mathers C. The global burden of cerebrovascular disease. Available at: http://www.who.int/healthinfo/statistics/bod_cerebrovasculardiseasestrok.... Accessed January 10, 2013
-
- Go AS, Mozaffarian D, Roger VL, et al. Executive summary: Heart disease and stroke statistics—2013 update: A report from the American Heart Association. Circulation 2013; 127: 143– 52 - PubMed
-
- Kleindorfer D, Lindsell CJ, Brass L, et al. National US estimates of recombinant tissue plasminogen activator use: ICD-9 codes substantially underestimate. Stroke 2008; 39: 924– 28 - PubMed
-
- Singer OC, Hamann GF, Misselwitz B, et al. Time trends in systemic thrombolysis in a large hospital-based stroke registry. Cerebrovasc Dis 2012; 33: 316– 21 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
