

Geography and the Medicaid mental health care infrastructure: implications for health care reform
- PMID: 23965816
- PMCID: PMC4048197
- DOI: 10.1001/jamapsychiatry.2013.377
Geography and the Medicaid mental health care infrastructure: implications for health care reform
Abstract
Importance: Medicaid is the largest payer of mental health (MH) care in the United States, and this role will increase among states that opt into the Medicaid expansion. However, owing to the dearth of MH care providers who accept Medicaid, expanded coverage may not increase access to services. Facilities that provide specialty outpatient MH services and accept Medicaid compose the backbone of the community-based treatment infrastructure for Medicaid enrollees. For states that opt into the expansion, it is important to understand which local communities may face the greatest barriers to access these facilities.
Objective: To examine the availability of outpatient MH facilities that accept Medicaid across US counties and whether specific types of communities are more likely to lack this infrastructure.
Design, setting, and participants: Data from the 2008 National Survey of Mental Health Treatment Facilities and Area Resource File were merged. A generalized ordered logistic regression with state fixed effects was estimated to examine determinants of accessibility of these facilities. Covariates included the percentages of residents who are black, Hispanic, living in poverty, and living in a rural area.
Main outcomes and measures: An ordered variable assessed whether a county had no access to outpatient MH facilities that accept Medicaid, intermediate access to these facilities (ie, ≥1 facility, but not top quintile of facility to Medicaid enrollee per capita ratio), or high access (ie, top quintile of facility to Medicaid enrollee per capita ratio).
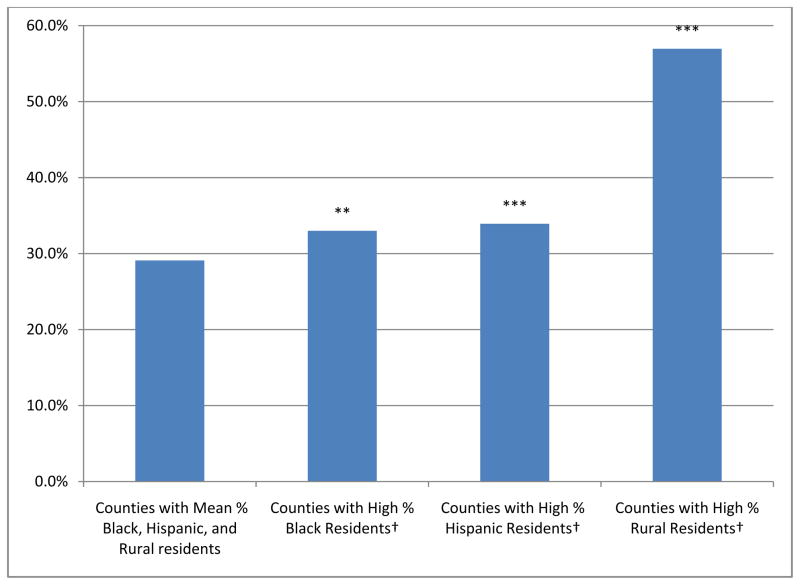
Results: More than one-third of counties do not have any outpatient MH facilities that accept Medicaid. Communities with a larger percentage of residents who are black (marginal effect [ME] = 3.9%; 95% CI, 1.2%-6.6%), Hispanic (ME = 4.8%; 95% CI, 2.3%-7.4%), or living in a rural area (ME = 27.9%; 95% CI, 25.3%-30.4%) are more likely to lack these facilities.
Conclusions and relevance: Many communities may face constraints on the MH safety-net system as Medicaid is expanded, especially rural communities and communities with a large percentage of black or Hispanic residents.
Conflict of interest statement
Figures
Comment in
-
Marginal Effects-Quantifying the Effect of Changes in Risk Factors in Logistic Regression Models.JAMA. 2019 Apr 2;321(13):1304-1305. doi: 10.1001/jama.2019.1954. JAMA. 2019. PMID: 30848814 No abstract available.
References
-
- Mark TL, Coffey RM, Vandivort-Warren R, Harwood HJ, King EC. U.S. spending for mental health and substance abuse treatment, 1991–2001. Health Aff (Millwood) 2005 Jan-Jun;(Suppl Web Exclusives):W5-133–W135-142. - PubMed
-
- Buck J, Miller K, Bae J. Mental Health and Substance Use Services in Medicaid, 1994. Rockville, MD: Center for Mental Health Service; 2000.
-
- Garfield RL, Zuvekas SH, Lave JR, Donohue JM. The impact of national health care reform on adults with severe mental disorders. Am J Psychiatry. 2011 May;168(5):486–494. - PubMed
-
- Kaiser Family Foundation. Medicaid and Children’s Health Insurance Program Revisions in the New Health Reform Law. Menlo Park, CA: Kaiser Family Foundation; 2010.
-
- Kaiser Family Foundation. A Guide to the Supreme Court’s Affordable Care Act Decision. Menlo Park, CA: Kaiser Family Foundation; 2012.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
