

The European medicines agency review of abiraterone for the treatment of metastatic castration-resistant prostate cancer in adult men after docetaxel chemotherapy and in chemotherapy-naive disease: summary of the scientific assessment of the committee for medicinal products for human use
- PMID: 23966222
- PMCID: PMC3780635
- DOI: 10.1634/theoncologist.2013-0092
The European medicines agency review of abiraterone for the treatment of metastatic castration-resistant prostate cancer in adult men after docetaxel chemotherapy and in chemotherapy-naive disease: summary of the scientific assessment of the committee for medicinal products for human use
Abstract
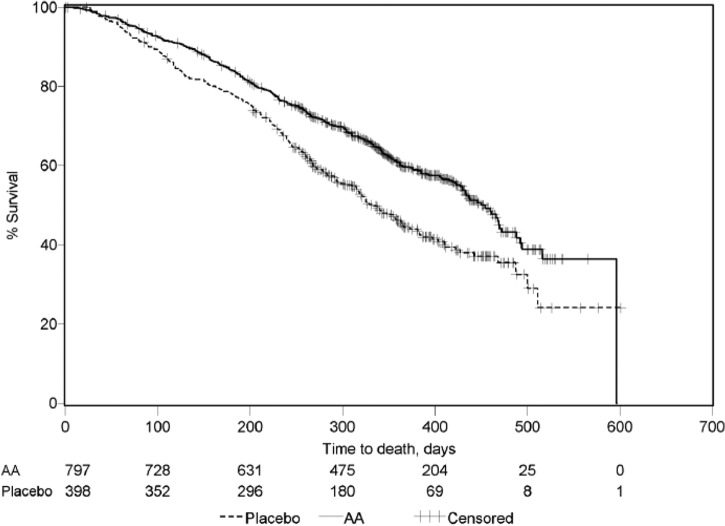
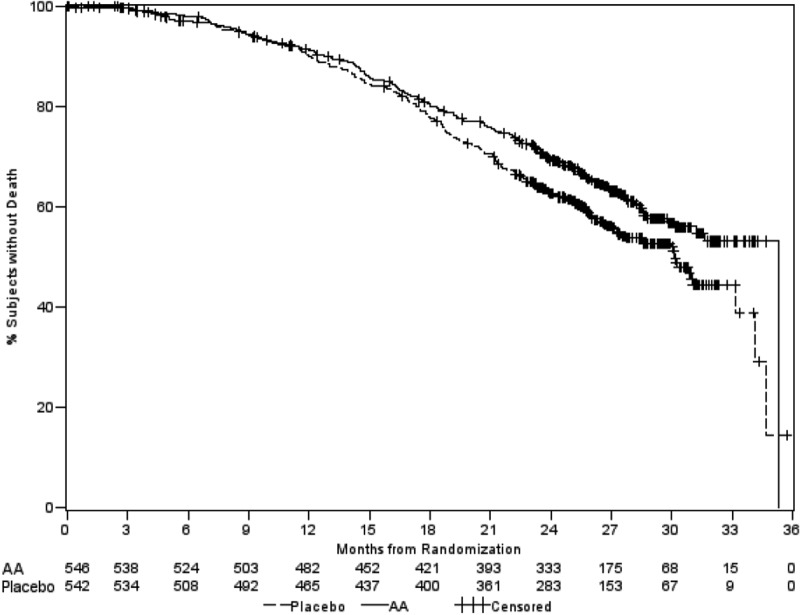
On September 5, 2011, abiraterone was approved in the European Union in combination with prednisone or prednisolone for the treatment of metastatic castration-resistant prostate cancer (CRPC) in adult men whose disease has progressed on or after a docetaxel-based chemotherapy regimen. On December 18, 2012, the therapeutic indication was extended to include the use of abiraterone in combination with prednisone or prednisolone for the treatment of metastatic CRPC in adult men who are asymptomatic or mildly symptomatic after failure of androgen deprivation therapy in whom chemotherapy is not yet clinically indicated. Abiraterone is a selective, irreversible inhibitor of cytochrome P450 17α, an enzyme that is key in the production of androgens. Inhibition of androgen biosynthesis deprives prostate cancer cells from important signals for growth, even in cases of resistance to castration. At the time of European Union approval and in a phase III trial in CRPC patients who had failed at least one docetaxel-based chemotherapy regimen, median overall survival for patients treated with abiraterone was 14.8 months versus 10.9 months for those receiving placebo (hazard ratio, 0.65; 95% confidence interval 0.54-0.77; p < .0001). In a subsequent phase III trial in a similar but chemotherapy-naïve patient population, median radiographic progression-free survival was 16.5 months for patients in the abiraterone treatment arm versus 8.3 months for patients in the placebo arm (hazard ratio, 0.53; 95% confidence interval, 0.45-0.62; p < .0001). Abiraterone was most commonly associated with adverse reactions resulting from increased or excessive mineralocorticoid activity. These were generally manageable with basic medical interventions. The most common side effects (affecting more than 10% of patients) were urinary tract infection, hypokalemia, hypertension, and peripheral edema.
Keywords: Abiraterone; EMA; European Medicines Agency; Prostate cancer.
Conflict of interest statement
Disclosures of potential conflicts of interest may be found at the end of this article.
Figures


References
-
- WHO. Global status report on noncommunicable diseases 2010. [Accessed August 18, 2013]. Available at www.who.int/nmh/publications/ncd_report_chapter1.pdf.
-
- Tannock IF, de Wit R, Berry WR, et al. TAX 327 Investigators. Docetaxel plus prednisone or mitoxantrone plus prednisone for advanced prostate cancer. N Engl J Med. 2004;351:1502–1512. - PubMed
-
- Pean E, Demolis P, Moreau A, et al. The European Medicines Agency review of cabazitaxel (Jevtana®) for the treatment of hormone-refractory metastatic prostate cancer: Summary of the scientific assessment of the committee for medicinal products for human use. The Oncologist. 2012;17:543–549. - PMC - PubMed
-
- Potter GA, Barrie SE, Jarman M, et al. Novel steroidal inhibitors of human cytochrome P45017α (17α-hydroxylase-C17,20-lyase): Potential agents for the treatment of prostatic cancer. J Med Chem. 1995;38:2463–2471. - PubMed
-
- Jarman M, Barrie SE, Llera JM. The 16,17-double bond is needed for irreversible inhibition of human cytochrome p45017α by abiraterone (17-(3-pyridyl)androsta-5, 16-dien-3beta-ol) and related steroidal inhibitors. J Med Chem. 1998;41:5375–5381. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
