

Pancreatic β-cell function is a stronger predictor of changes in glycemic control after an aerobic exercise intervention than insulin sensitivity
- PMID: 23966244
- PMCID: PMC3790622
- DOI: 10.1210/jc.2013-2232
Pancreatic β-cell function is a stronger predictor of changes in glycemic control after an aerobic exercise intervention than insulin sensitivity
Abstract
Context: Understanding intersubject variability in glycemic control following exercise training will help individualize treatment.
Objective: Our aim was to determine whether this variability is related to training-induced changes in insulin sensitivity or pancreatic β-cell function.
Design, setting, and participants: We conducted an observational clinical study of 105 subjects with impaired glucose tolerance or type 2 diabetes.
Interventions and main outcome measures: Individual subject changes in fitness (VO2max), glycemia (glycosylated hemoglobin, fasting glucose, oral glucose tolerance test), insulin sensitivity (hyperinsulinemic-euglycemic clamp), oral glucose-stimulated insulin secretion (GSIS), and disposition index (DI) were measured following 12 to 16 weeks of aerobic exercise training. Regression analyses were used to identify relationships between variables.
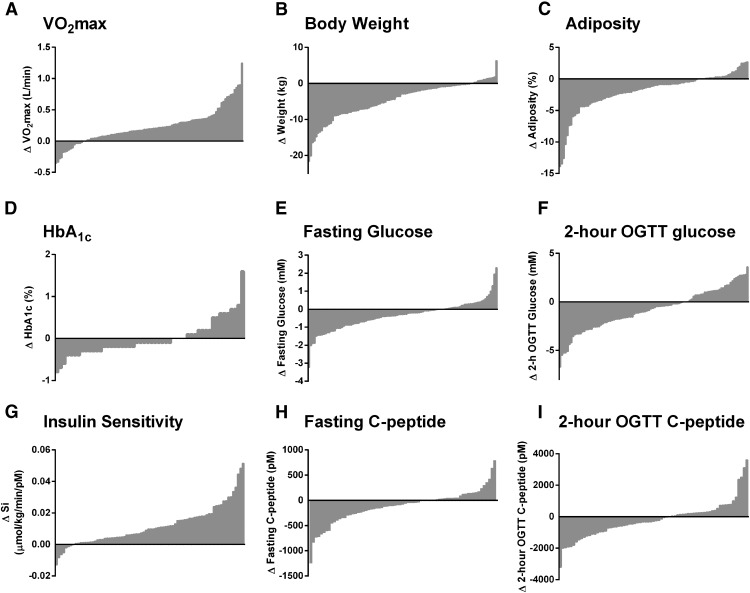
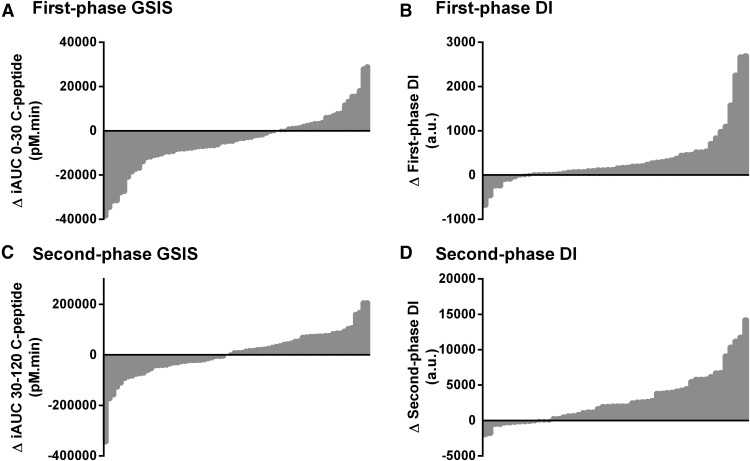
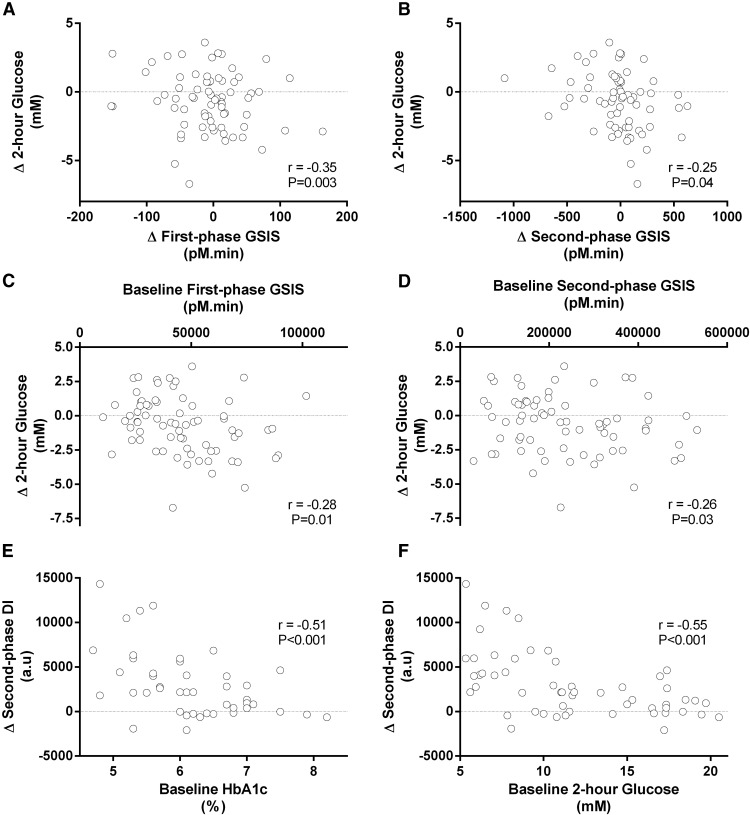
Results: After training, 86% of subjects increased VO2max and lost weight. Glycosylated hemoglobin, fasting glucose, and 2-hour oral glucose tolerance test were reduced in 69%, 62%, and 68% of subjects, respectively, while insulin sensitivity improved in 90% of the participants. Changes in glycemic control were congruent with changes in GSIS such that 66% of subjects had a reduction in first-phase GSIS, and 46% had reduced second-phase GSIS. Training increased first- and second-phase DI in 83% and 74% of subjects. Training-induced changes in glycemic control were related to changes in GSIS (P < .05), but not insulin sensitivity or DI, and training-induced improvements in glycemic control were largest in subjects with greater pretraining GSIS.
Conclusions: Intersubject variability in restoring glycemic control following exercise is explained primarily by changes in insulin secretion. Thus, baseline and training-induced changes in β-cell function may be a key determinant of training-induced improvements in glycemic control.
Trial registration: ClinicalTrials.gov NCT01234155.
Figures
References
-
- Pan XR, Li GW, Hu YH, et al. Effects of diet and exercise in preventing NIDDM in people with impaired glucose tolerance. The Da Qing IGT and Diabetes Study. Diabetes Care. 1997;20(4):537–544 - PubMed
-
- Balducci S, Zanuso S, Nicolucci A, et al. , Italian Diabetes and Exercise Study (IDES) Investigators Effect of an intensive exercise intervention strategy on modifiable cardiovascular risk factors in subjects with type 2 diabetes mellitus: a randomized controlled trial: the Italian Diabetes and Exercise Study (IDES). Arch Intern Med. 2010;170(20):1794–1803 - PubMed
-
- Sigal RJ, Kenny GP, Boulé NG, et al. Effects of aerobic training, resistance training, or both on glycemic control in type 2 diabetes: a randomized trial. Ann Intern Med. 2007;147(6):357–369 - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
