

Priorities in pediatric epilepsy research: improving children's futures today
- PMID: 23966254
- PMCID: PMC3795602
- DOI: 10.1212/WNL.0b013e3182a55fb9
Priorities in pediatric epilepsy research: improving children's futures today
Abstract
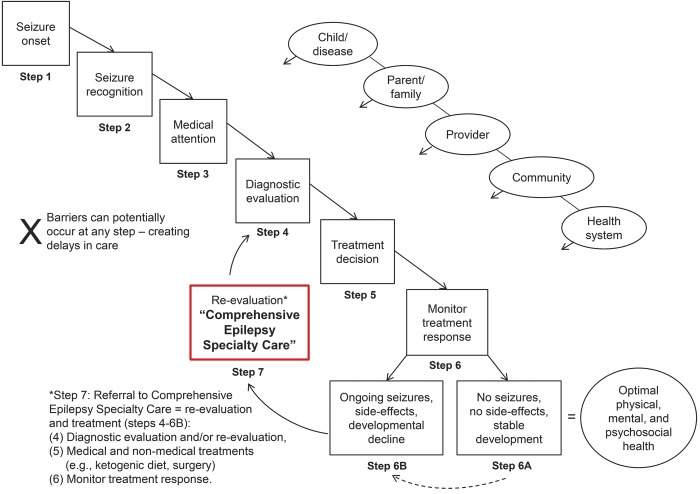
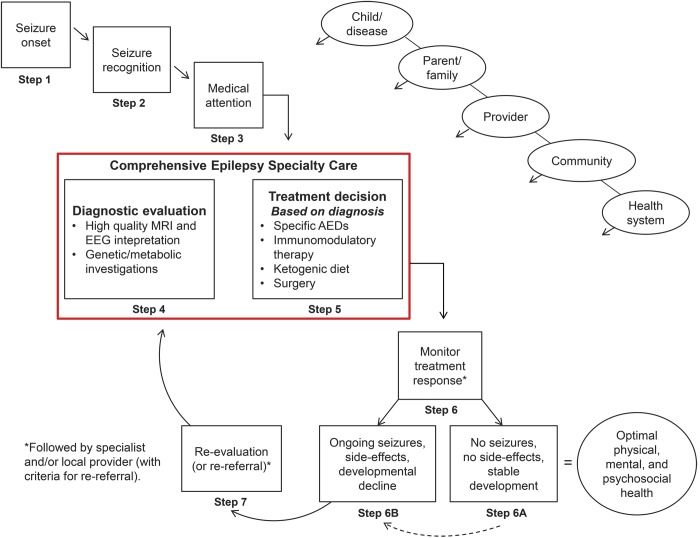
The Priorities in Pediatric Epilepsy Research workshop was held in the spirit of patient-centered and patient-driven mandates for developing best practices in care, particularly for epilepsy beginning under age 3 years. The workshop brought together parents, representatives of voluntary advocacy organizations, physicians, allied health professionals, researchers, and administrators to identify priority areas for pediatric epilepsy care and research including implementation and testing of interventions designed to improve care processes and outcomes. Priorities highlighted were 1) patient outcomes, especially seizure control but also behavioral, academic, and social functioning; 2) early and accurate diagnosis and optimal treatment; 3) role and involvement of parents (communication and shared decision-making); and 4) integration of school and community organizations with epilepsy care delivery. Key factors influencing pediatric epilepsy care included the child's impairments and seizure presentation, parents, providers, the health care system, and community systems. Care was represented as a sequential process from initial onset of seizures to referral for comprehensive evaluation when needed. We considered an alternative model in which comprehensive care would be utilized from onset, proactively, rather than reactively after pharmacoresistance became obvious. Barriers, including limited levels of evidence about many aspects of diagnosis and management, access to care--particularly epilepsy specialty and behavioral health care--and implementation, were identified. Progress hinges on coordinated research efforts that systematically address gaps in knowledge and overcoming barriers to access and implementation. The stakes are considerable, and the potential benefits for reduced burden of refractory epilepsy and lifelong disabilities may be enormous.
Figures
References
-
- Institute of Medicine Epilepsy Across the Spectrum: Promoting Health and Understanding. Washington, DC: The National Academies Press; 2012 - PubMed
-
- Berg AT, Shinnar S, Levy SR, Testa F, Smith-Rapaport S, Beckerman B. Early development of intractable epilepsy in children: a prospective study. Neurology 2001;56:1445–1452 - PubMed
-
- Camfield CS, Camfield PR, Gordon K, Wirrell E, Dooley JM. Incidence of epilepsy in childhood and adolescence: a population-based study in Nova Scotia from 1977 to 1985. Epilepsia 1996;37:19–23 - PubMed
-
- Olafsson E, Hauser WA, Ludvigsson P, Gudmundsson G. Incidence of epilepsy in rural Iceland: a population-based study. Epilepsia 1996;37:951–955 - PubMed
-
- Camfield P, Camfield C. Long-term prognosis for symptomatic (secondarily) generalized epilepsies: a population-based study. Epilepsia 2007;48:1128–1132 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical