

Multidetector CT findings in patients with mesenteric ischaemia following cardiopulmonary bypass surgery
- PMID: 23966376
- PMCID: PMC3798331
- DOI: 10.1259/bjr.20130277
Multidetector CT findings in patients with mesenteric ischaemia following cardiopulmonary bypass surgery
Abstract
Objective: To investigate CT findings in patients with pathologically proven mesenteric ischaemia post-cardiopulmonary bypass surgery and compare them with the control group of patients without ischaemia.
Methods: 68 patients were identified by a search of local surgical and pathological databases; these patients met the inclusion criteria of a laparotomy within 1 month of a procedure requiring cardiopulmonary bypass and a CT abdomen/pelvis within 1 week of the pathological diagnosis. Two radiologists independently reviewed the studies, evaluating 17 separate findings relating to the bowel, the vasculature or other structures; consensus was subsequently reached. The diagnostic value of CT findings was assessed using logistic regression.
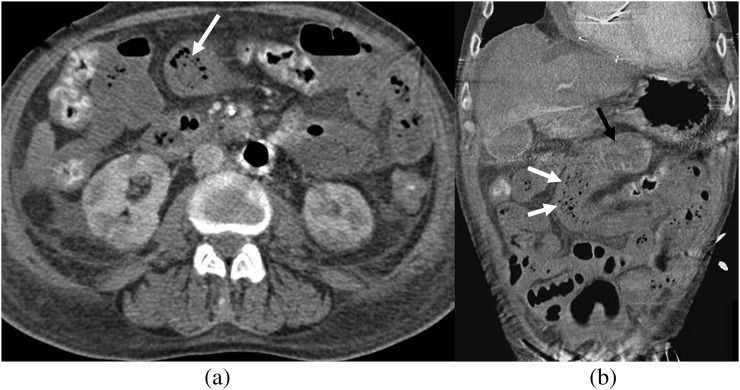
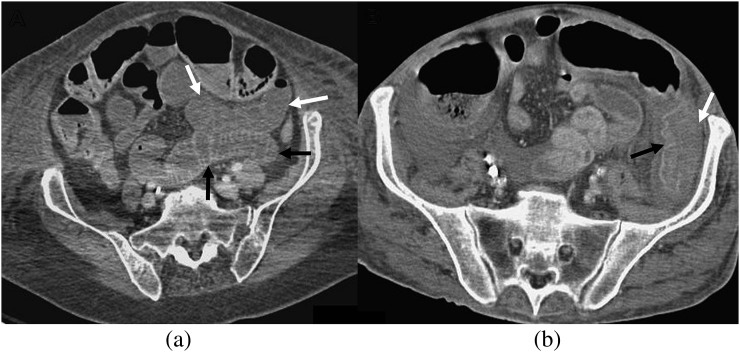
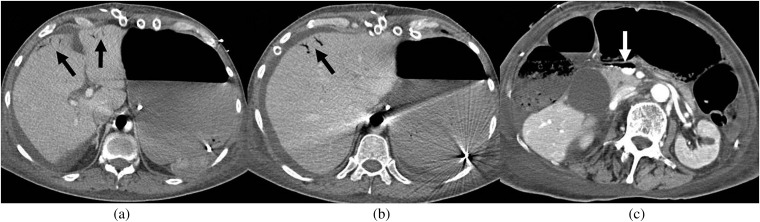
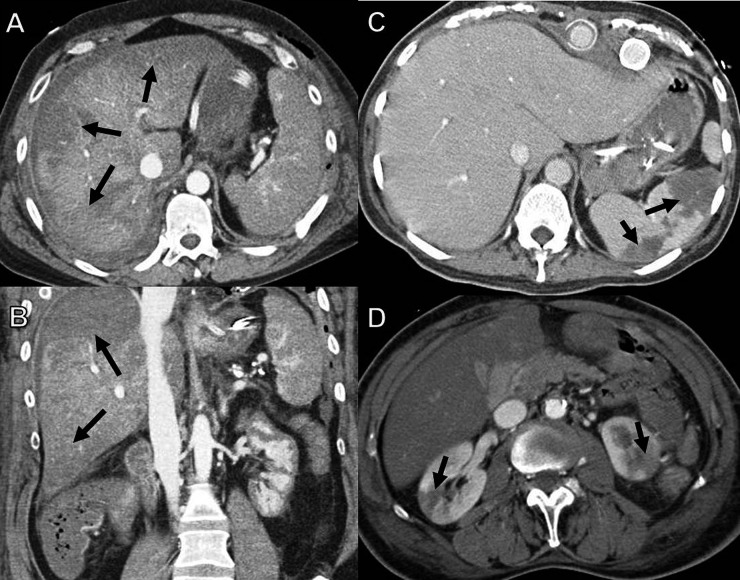
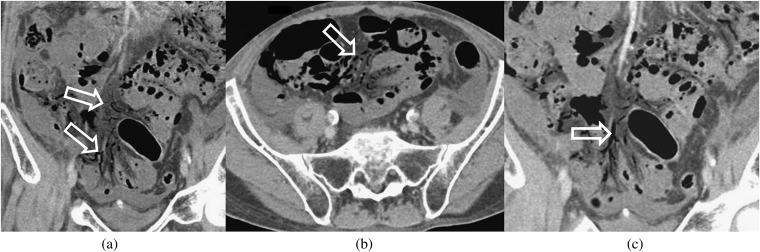
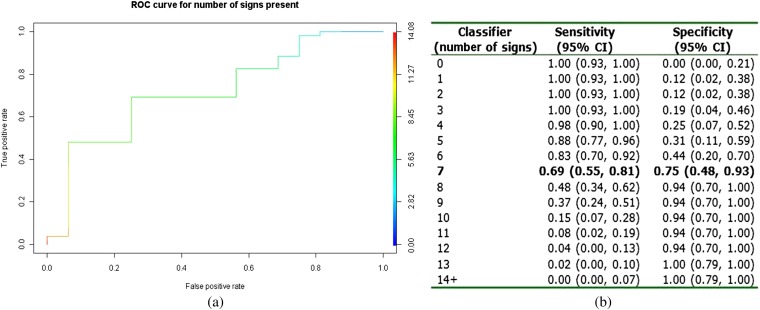
Results: 52 of 68 patients had pathologically proven ischaemia. Portal venous gas, mesenteric venous gas and small bowel faeces sign all had specificities of >0.94 for ischaemia but low sensitivity (<0.27). Differential mural enhancement had high sensitivity (0.92) but poor specificity (0.50). The combination of pneumatosis, bowel loop dilatation and differential mural enhancement predicted bowel ischaemia with a probability of 98%. The hardest signs to interpret based on poor interreader kappa agreement were bowel wall thinning, mesenteric stranding and differential mural enhancement.
Conclusion: A combination of CT signs was predictive of ischaemic bowel; however, the more specific findings lacked sensitivity. If clinical suspicion is high for bowel ischaemia, prompt surgical intervention is warranted, regardless of CT findings.
Advances in knowledge: Arterial occlusion was uncommon and venous occlusion was not present, which is supportive of a predominantly non-occlusive aetiology for ischaemia in this patient group.
Figures


References
-
- Allen KB, Salam AA, Lumsden AB. Acute mesenteric ischemia after cardiopulmonary bypass. J Vasc Surg 1992;16:391–6 - PubMed
-
- Venkateswaran RV, Charman SC, Goddard M, Large SR. Lethal mesenteric ischaemia after cardiopulmonary bypass: a common complication? Eur J Cardiothorac Surg 2002;22:534–8 - PubMed
-
- Nonthasoot B, Tullavardhana T, Sirichindakul B, Suphapol J, Nivatvongs S. Acute mesenteric ischemia: still high mortality rate in the era of 24-hour availability of angiography. J Med Assoc Thai 2005;88:S46–50 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
