

Diarrhea in early childhood: short-term association with weight and long-term association with length
- PMID: 23966558
- PMCID: PMC3783094
- DOI: 10.1093/aje/kwt094
Diarrhea in early childhood: short-term association with weight and long-term association with length
Abstract
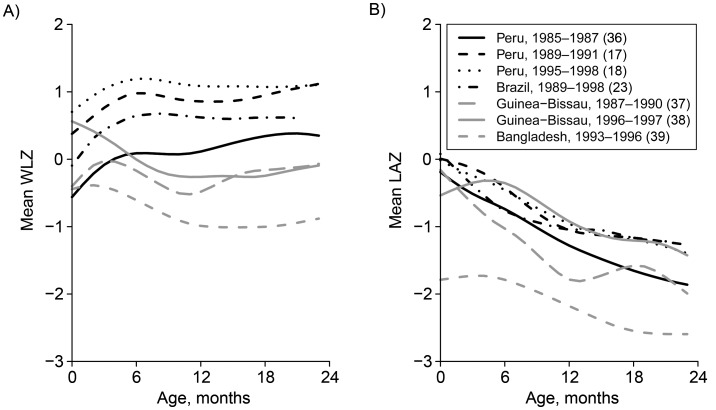
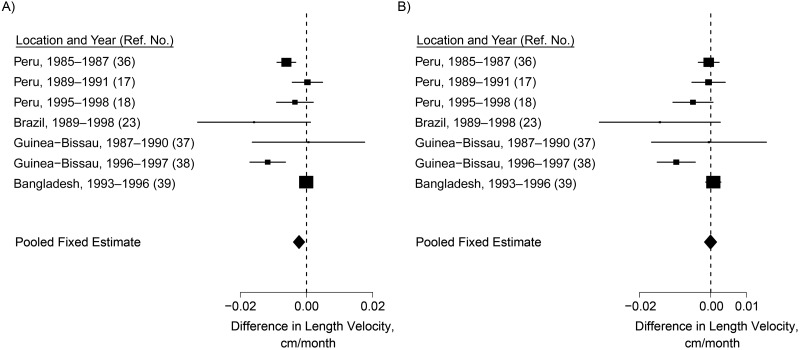
The short-term association between diarrhea and weight is well-accepted, but the long-term association between diarrhea and growth is less clear. Using data from 7 cohort studies (Peru, 1985-1987; Peru, 1989-1991; Peru, 1995-1998; Brazil, 1989-1998; Guinea-Bissau, 1987-1990; Guinea-Bissau, 1996-1997; and Bangladesh, 1993-1996), we evaluated the lagged relationship between diarrhea and growth in the first 2 years of life. Our analysis included 1,007 children with 597,638 child-days of diarrhea surveillance and 15,629 anthropometric measurements. We calculated the associations between varying diarrhea burdens during lagged 30-day periods and length at 24 months of age. The cumulative association between the average diarrhea burden and length at age 24 months was -0.38 cm (95% confidence interval: -0.59, -0.17). Diarrhea during the 30 days prior to anthropometric measurement was consistently associated with lower weight at most ages, but there was little indication of a short-term association with length. Diarrhea was associated with a small but measurable decrease in linear growth over the long term. These findings support a focus on prevention of diarrhea as part of an overall public health strategy for improving child health and nutrition; however, more research is needed to explore catch-up growth and potential confounders.
Keywords: child health; diarrhea; malnutrition; stunting; wasting.
Figures







References
-
- Keusch GT, Fontaine O, Bhargava A, et al. Disease Control Priorities in Developing Countries. 2nd ed. New York, NY: Oxford University Press; 2006. Diarrheal diseases; pp. 371–388.
-
- Martorell R, Habicht JP, Yarbrough C, et al. Acute morbidity and physical growth in rural Guatemalan children. Am J Dis Child. 1975;129(11):1296–1301. - PubMed
-
- Cole TJ, Parkin JM. Infection and its effect on the growth of young children: a comparison of The Gambia and Uganda. Trans R Soc Trop Med Hyg. 1977;71(3):196–198. - PubMed
-
- Guerrant RL, Kirchhoff LV, Shields DS, et al. Prospective study of diarrheal illnesses in northeastern Brazil: patterns of disease, nutritional impact, etiologies, and risk factors. J Infect Dis. 1983;148(6):986–997. - PubMed
-
- Black RE, Brown KH, Becker S. Effects of diarrhea associated with specific enteropathogens on the growth of children in rural Bangladesh. Pediatrics. 1984;73(6):799–805. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
