

Towards universal voluntary HIV testing and counselling: a systematic review and meta-analysis of community-based approaches
- PMID: 23966838
- PMCID: PMC3742447
- DOI: 10.1371/journal.pmed.1001496
Towards universal voluntary HIV testing and counselling: a systematic review and meta-analysis of community-based approaches
Abstract
Background: Effective national and global HIV responses require a significant expansion of HIV testing and counselling (HTC) to expand access to prevention and care. Facility-based HTC, while essential, is unlikely to meet national and global targets on its own. This article systematically reviews the evidence for community-based HTC.
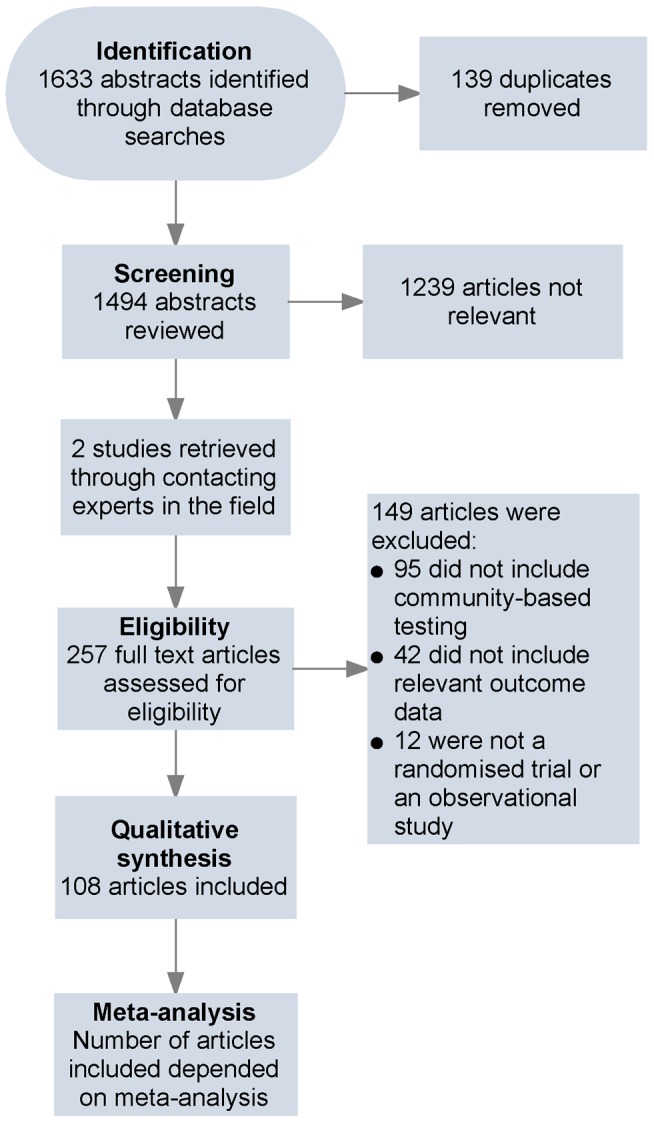
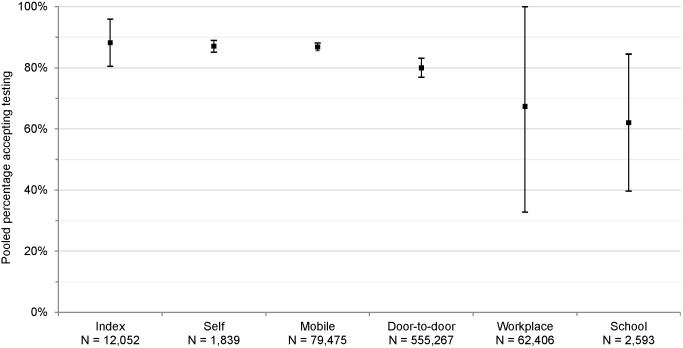
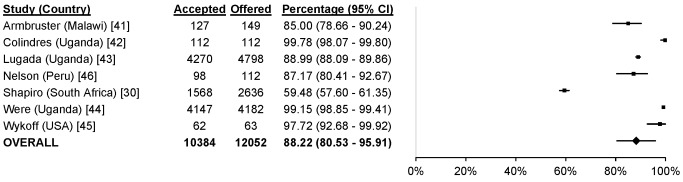
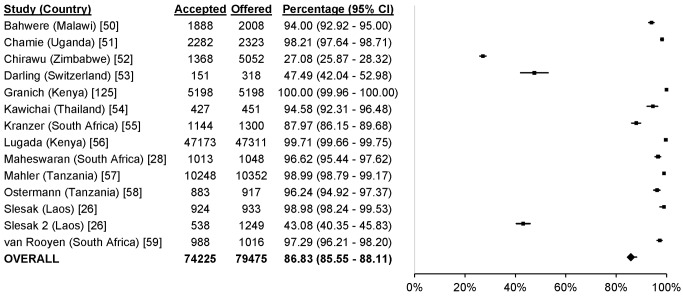
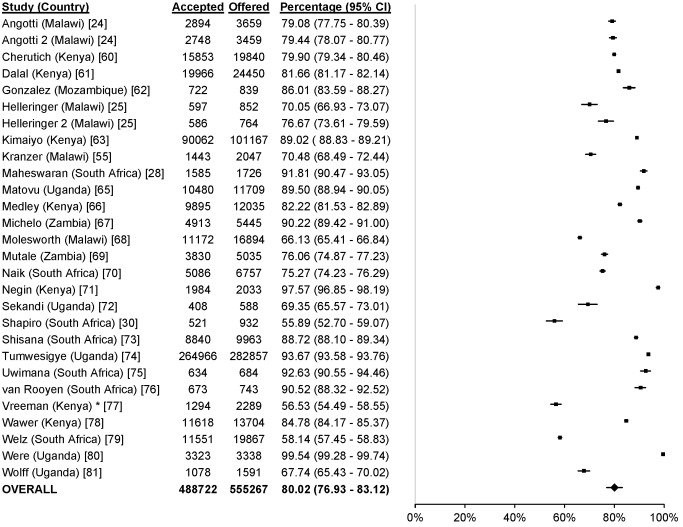
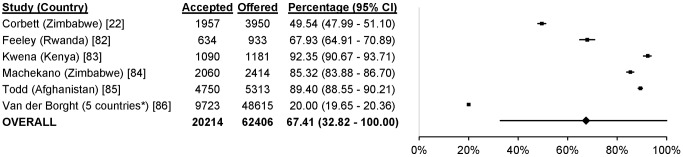
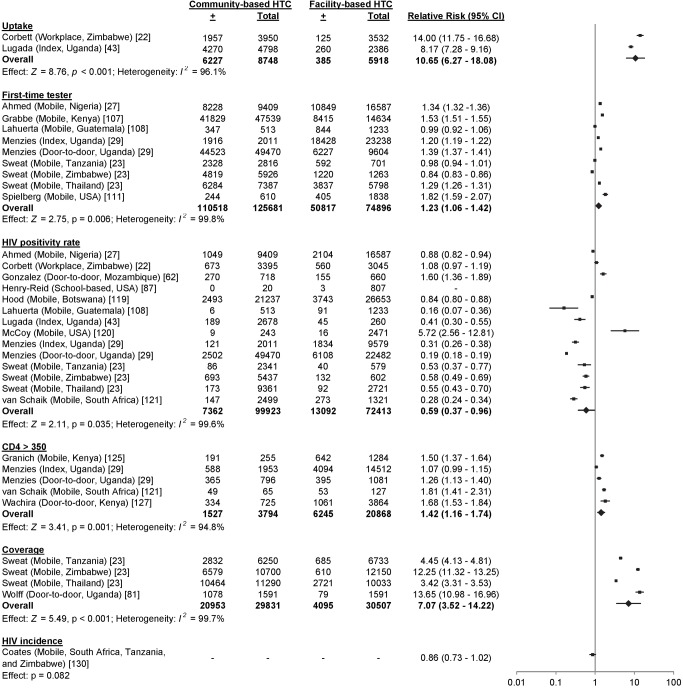
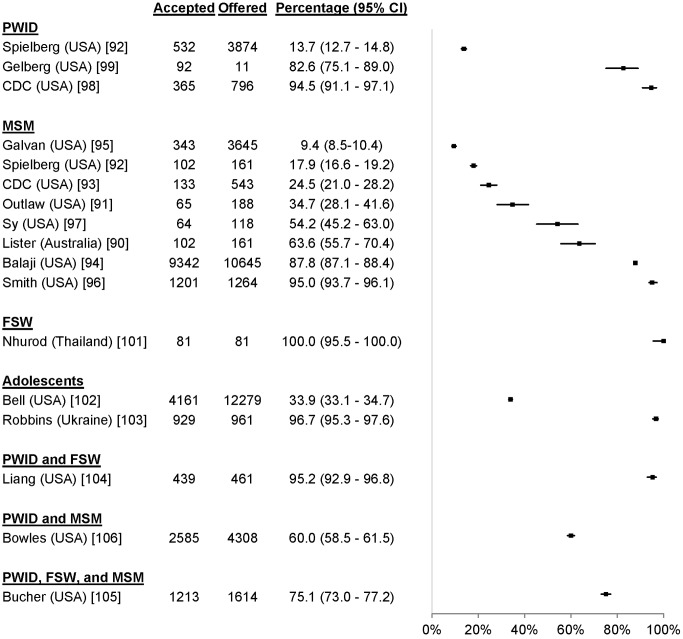
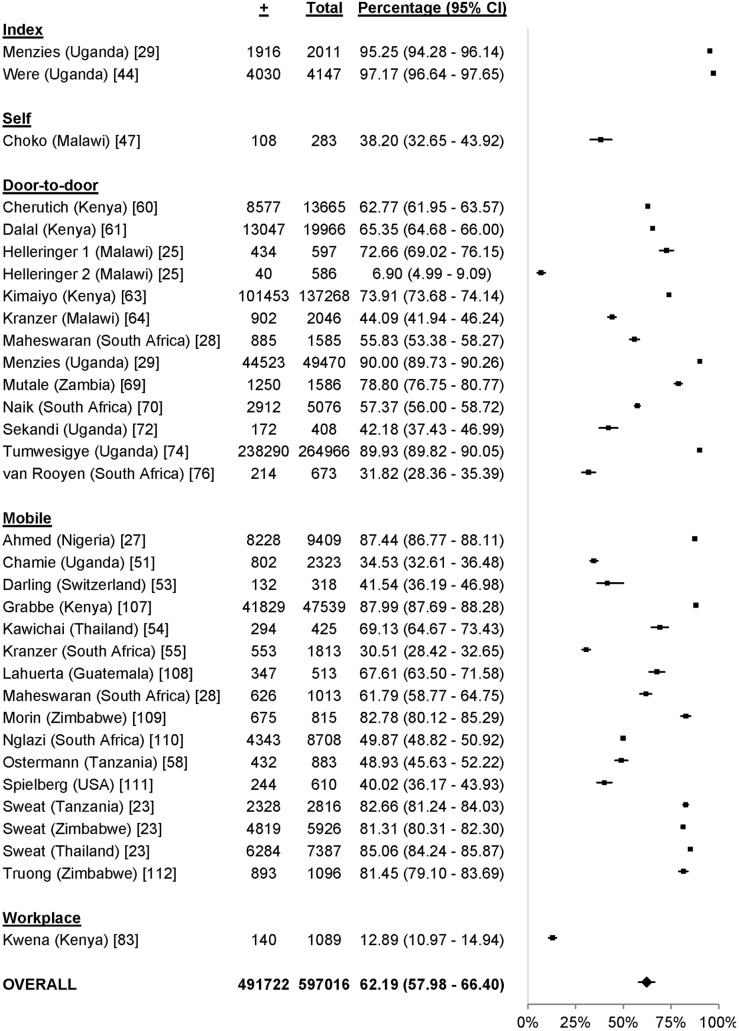
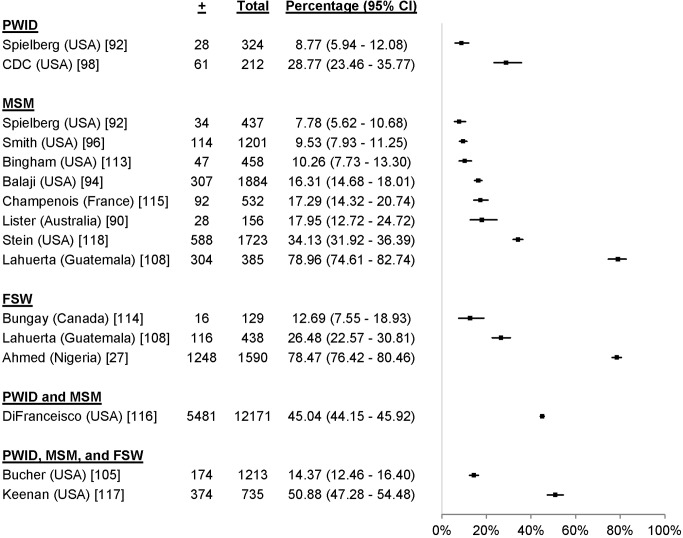
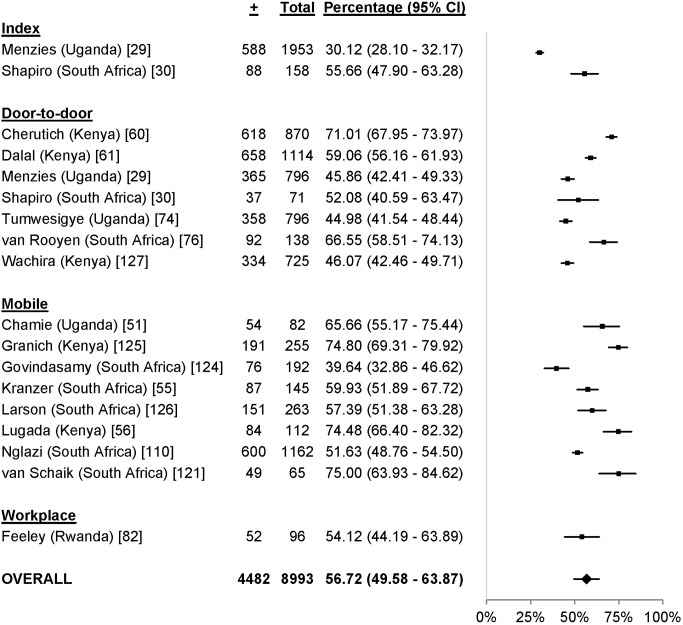
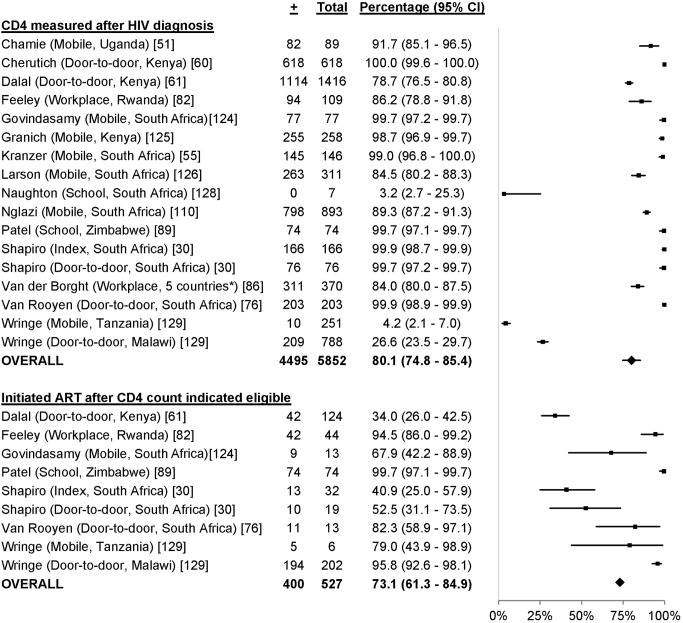
Methods and findings: PubMed was searched on 4 March 2013, clinical trial registries were searched on 3 September 2012, and Embase and the World Health Organization Global Index Medicus were searched on 10 April 2012 for studies including community-based HTC (i.e., HTC outside of health facilities). Randomised controlled trials, and observational studies were eligible if they included a community-based testing approach and reported one or more of the following outcomes: uptake, proportion receiving their first HIV test, CD4 value at diagnosis, linkage to care, HIV positivity rate, HTC coverage, HIV incidence, or cost per person tested (outcomes are defined fully in the text). The following community-based HTC approaches were reviewed: (1) door-to-door testing (systematically offering HTC to homes in a catchment area), (2) mobile testing for the general population (offering HTC via a mobile HTC service), (3) index testing (offering HTC to household members of people with HIV and persons who may have been exposed to HIV), (4) mobile testing for men who have sex with men, (5) mobile testing for people who inject drugs, (6) mobile testing for female sex workers, (7) mobile testing for adolescents, (8) self-testing, (9) workplace HTC, (10) church-based HTC, and (11) school-based HTC. The Newcastle-Ottawa Quality Assessment Scale and the Cochrane Collaboration's "risk of bias" tool were used to assess the risk of bias in studies with a comparator arm included in pooled estimates. 117 studies, including 864,651 participants completing HTC, met the inclusion criteria. The percentage of people offered community-based HTC who accepted HTC was as follows: index testing, 88% of 12,052 participants; self-testing, 87% of 1,839 participants; mobile testing, 87% of 79,475 participants; door-to-door testing, 80% of 555,267 participants; workplace testing, 67% of 62,406 participants; and school-based testing, 62% of 2,593 participants. Mobile HTC uptake among key populations (men who have sex with men, people who inject drugs, female sex workers, and adolescents) ranged from 9% to 100% (among 41,110 participants across studies), with heterogeneity related to how testing was offered. Community-based approaches increased HTC uptake (relative risk [RR] 10.65, 95% confidence interval [CI] 6.27-18.08), the proportion of first-time testers (RR 1.23, 95% CI 1.06-1.42), and the proportion of participants with CD4 counts above 350 cells/µl (RR 1.42, 95% CI 1.16-1.74), and obtained a lower positivity rate (RR 0.59, 95% CI 0.37-0.96), relative to facility-based approaches. 80% (95% CI 75%-85%) of 5,832 community-based HTC participants obtained a CD4 measurement following HIV diagnosis, and 73% (95% CI 61%-85%) of 527 community-based HTC participants initiated antiretroviral therapy following a CD4 measurement indicating eligibility. The data on linking participants without HIV to prevention services were limited. In low- and middle-income countries, the cost per person tested ranged from US$2-US$126. At the population level, community-based HTC increased HTC coverage (RR 7.07, 95% CI 3.52-14.22) and reduced HIV incidence (RR 0.86, 95% CI 0.73-1.02), although the incidence reduction lacked statistical significance. No studies reported any harm arising as a result of having been tested.
Conclusions: Community-based HTC achieved high rates of HTC uptake, reached people with high CD4 counts, and linked people to care. It also obtained a lower HIV positivity rate relative to facility-based approaches. Further research is needed to further improve acceptability of community-based HTC for key populations. HIV programmes should offer community-based HTC linked to prevention and care, in addition to facility-based HTC, to support increased access to HIV prevention, care, and treatment.
Review registration: International Prospective Register of Systematic Reviews CRD42012002554 Please see later in the article for the Editors' Summary.
Conflict of interest statement
The authors have declared that no competing interests exist. The opinions and statements in this article are those of the authors and do not necessarily represent the official policy, endorsement, or views of their organisations.
Figures



References
-
- Murray CJ, Vos T, Lozano R, Naghavi M, Flaxman AD, et al. (2012) Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 380: 2197–2223. - PubMed
-
- Joint United Nations Programme on HIV/AIDS (2012) UNAIDS report on the global AIDS epidemic. Available: http://www.unaids.org/en/media/unaids/contentassets/documents/epidemiolo.... Accessed 25 July 2013.
-
- United Nations General Assembly (2011) Political declaration on HIV/AIDS: intensifying our efforts to eliminate HIV/AIDS. Available: http://www.unaids.org/en/media/unaids/contentassets/documents/document/2.... Accessed 1 July 2013.
-
- World Health Organization (2007) Guidance on provider-initiated HIV testing and counselling in health facilities. Available: http://whqlibdoc.who.int/publications/2007/9789241595568_eng.pdf. Accessed 1 July 2013.
-
- Roura M, Watson-Jones D, Kahawita TM, Ferguson L, Ross DA (2013) Provider-initiated testing and counselling programmes in sub-Saharan Africa: a systematic review of their operational implementation. AIDS 27: 617–626. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
