

Acute measles encephalitis in partially vaccinated adults
- PMID: 23967232
- PMCID: PMC3742472
- DOI: 10.1371/journal.pone.0071671
Acute measles encephalitis in partially vaccinated adults
Abstract
Background: The pathogenesis of acute measles encephalitis (AME) is poorly understood. Treatment with immune-modulators is based on theories that post-infectious autoimmune responses cause demyelination. The clinical course and immunological parameters of AME were examined during an outbreak in Vietnam.
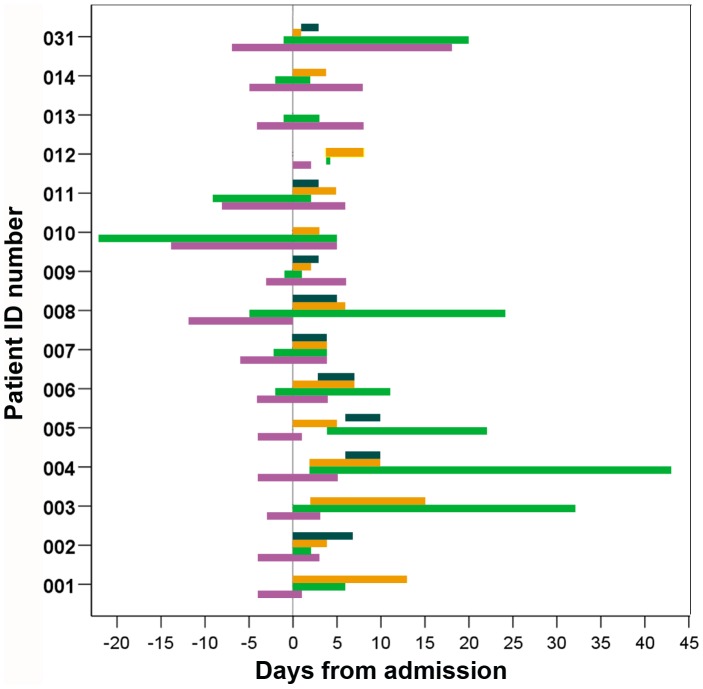
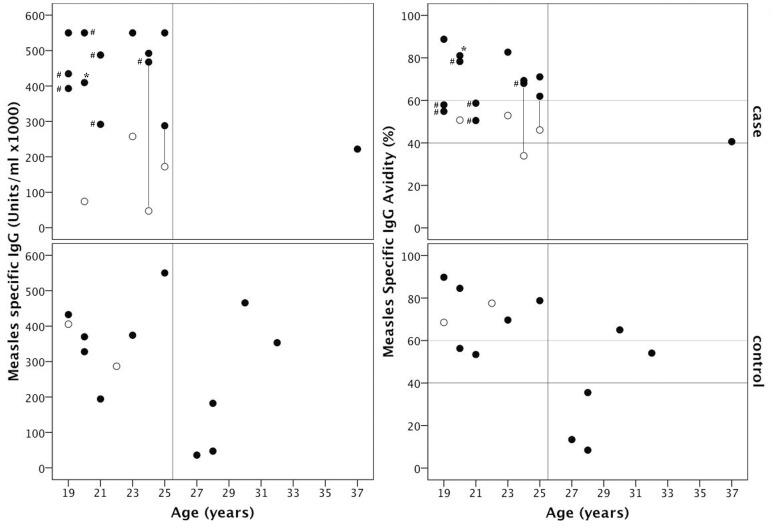
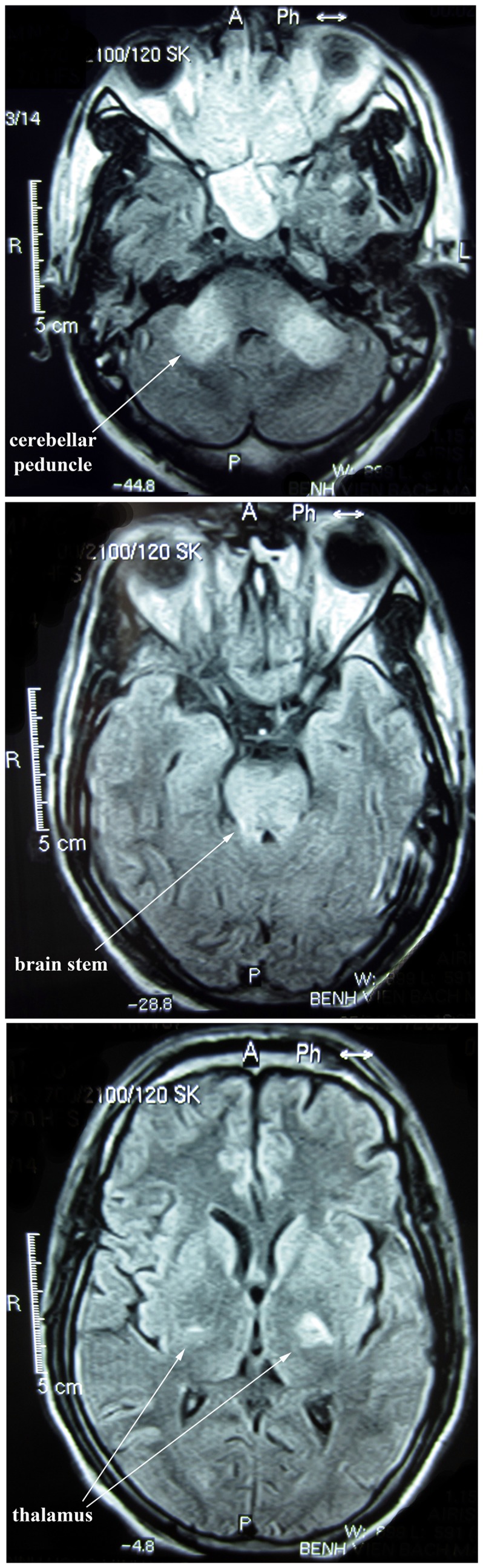
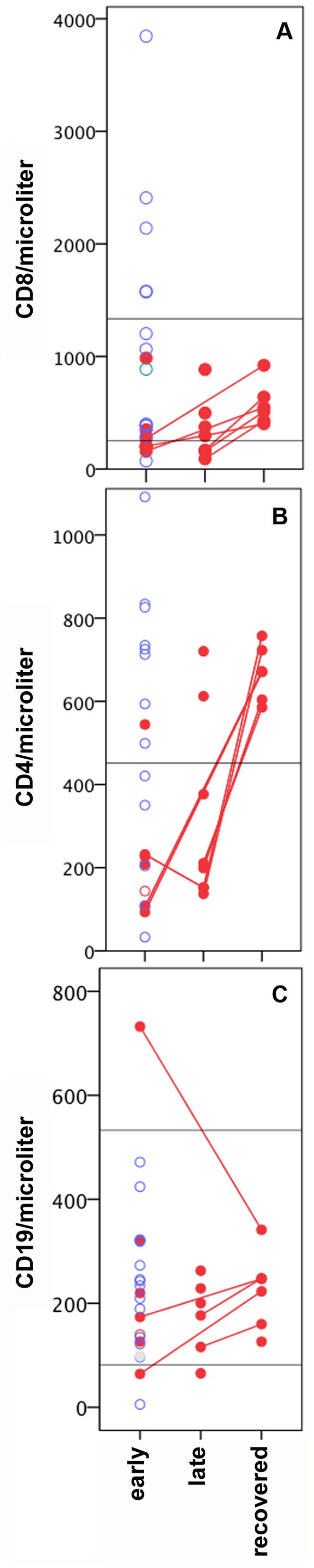
Methods and findings: Fifteen measles IgM-positive patients with confusion or Glasgow Coma Scale (GCS) score below 13, and thirteen with uncomplicated measles were enrolled from 2008-2010. Standardized clinical exams were performed and blood collected for lymphocyte and measles- and auto-antibody analysis. The median age of AME patients was 21 years, similar to controls. Eleven reported receiving measles vaccination when aged one year. Confusion developed a median of 4 days after rash. Six patients had GCS <8 and four required mechanical ventilation. CSF showed pleocytosis (64%) and proteinorrhachia (71%) but measles virus RNA was not detected. MRI revealed bilateral lesions in the cerebellum and brain stem in some patients. Most received dexamethasone +/- IVIG within 4 days of admission but symptoms persisted for ≥3 weeks in five. The concentration of voltage gated calcium channel-complex-reactive antibodies was 900 pM in one patient, and declined to 609 pM ∼ 3 months later. Measles-reactive IgG antibody avidity was high in AME patients born after vaccine coverage exceeded 50% (∼ 25 years earlier). AME patients had low CD4 (218/µl, p = 0.029) and CD8 (200/µl, p = 0.012) T-cell counts compared to controls.
Conclusion: Young adults presenting with AME in Vietnam reported a history of one prior measles immunization, and those aged <25 years had high measles-reactive IgG avidity indicative of prior vaccination. This suggests that one-dose measles immunization is not sufficient to prevent AME in young adults and reinforces the importance of maintaining high coverage with a two-dose measles immunization schedule. Treatment with corticosteroids and IVIG is common practice, and should be assessed in randomized clinical trials.
Conflict of interest statement
Figures
References
-
- Wolfson LJ, Strebel PM, Gacic-Dobo M, Hoekstra EJ, McFarland JW, et al. (2007) Has the 2005 measles mortality reduction goal been achieved? A natural history modelling study. Lancet 369: 191–200. - PubMed
-
- Perry RT, Halsey NA (2004) The clinical significance of measles: a review. J Infect Dis 189 Suppl 1S4–16. - PubMed
-
- Schneider-Schaulies J, Niewiesk S, Schneider-Schaulies S, ter Meulen V (1999) Measles virus in the CNS: the role of viral and host factors for the establishment and maintenance of a persistent infection. J Neurovirol 5: 613–622. - PubMed
-
- Bellini WJ, Rota JS, Lowe LE, Katz RS, Dyken PR, et al. (2005) Subacute sclerosing panencephalitis: more cases of this fatal disease are prevented by measles immunization than was previously recognized. J Infect Dis 192: 1686–1693. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
