

Risk of angioedema following invasive or surgical procedures in HAE type I and II--the natural history
- PMID: 23968383
- PMCID: PMC4223932
- DOI: 10.1111/all.12186
Risk of angioedema following invasive or surgical procedures in HAE type I and II--the natural history
Abstract
Background: Hereditary angioedema (HAE), caused by deficiency in C1-inhibitor (C1-INH), leads to unpredictable edema of subcutaneous tissues with potentially fatal complications. As surgery can be a trigger for edema episodes, current guidelines recommend preoperative prophylaxis with C1-INH or attenuated androgens in patients with HAE undergoing surgery. However, the risk of an HAE attack in patients without prophylaxis has not been quantified.
Objectives: This analysis examined rates of perioperative edema in patients with HAE not receiving prophylaxis.
Methods: This was a retrospective analysis of records of randomly selected patients with HAE type I or II treated at the Frankfurt Comprehensive Care Centre. These were examined for information about surgical procedures and the presence of perioperative angioedema.
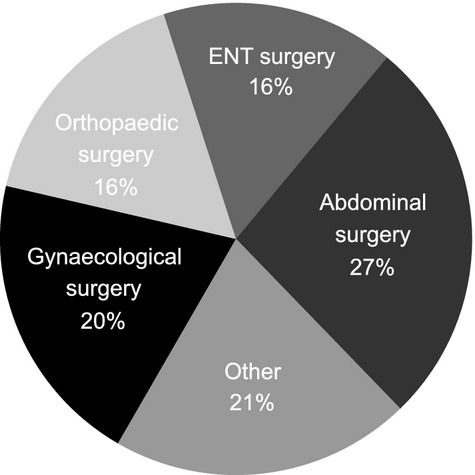
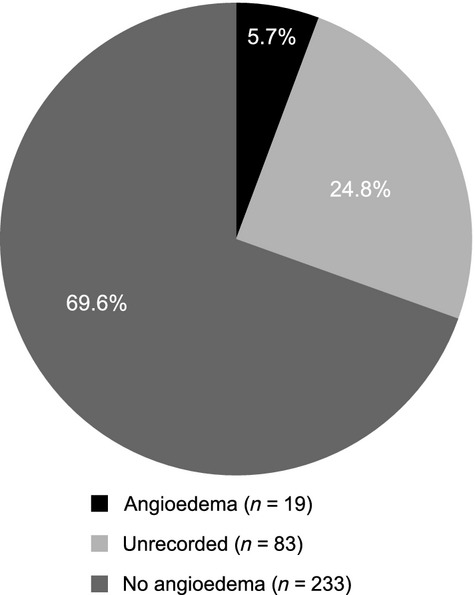
Results: A total of 331 patients were included; 247 underwent 700 invasive procedures. Of these procedures, 335 were conducted in 144 patients who had not received prophylaxis at the time of surgery. Categories representing significant numbers of procedures were abdominal (n = 113), ENT (n = 71), and gynecological (n = 58) procedures. The rate of documented angioedema without prophylaxis across all procedures was 5.7%; in 24.8% of procedures, the presence of perioperative angioedema could not be excluded, leading to a maximum potential risk of 30.5%. Predictors of perioperative angioedema could not be identified.
Conclusion: The risk of perioperative angioedema in patients with HAE type I or II without prophylaxis undergoing surgical procedures ranged from 5.7% to 30.5% (CI 3.5-35.7%). The unpredictability of HAE episodes supports current international treatment recommendations to consider short-term prophylaxis for all HAE patients undergoing surgery.
Keywords: C1-inhibitor deficiency; HAE; hereditary angioedema; preprocedure prophylaxis; surgical procedures.
© 2013 University Hospital Frankfurt, Goethe University. Allergy published by John Wiley & Sons Ltd.
Figures

References
-
- Agostoni A, Cicardi M. Replacement therapy in hereditary and acquired angioedema. Pharmacol Res. 1992;26(Suppl 2):148–149. - PubMed
-
- Davis AE., III C1 inhibitor and hereditary angioneurotic edema. Annu Rev Immunol. 1988;6:595–628. - PubMed
-
- Cicardi M, Johnson DT. Hereditary and acquired complement component 1 esterase inhibitor deficiency: a review for the hematologist. Acta Haematol. 2012;127:208–220. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
