

A patient with CKD and poor nutritional status
- PMID: 23970134
- PMCID: PMC3848406
- DOI: 10.2215/CJN.04630513
A patient with CKD and poor nutritional status
Abstract
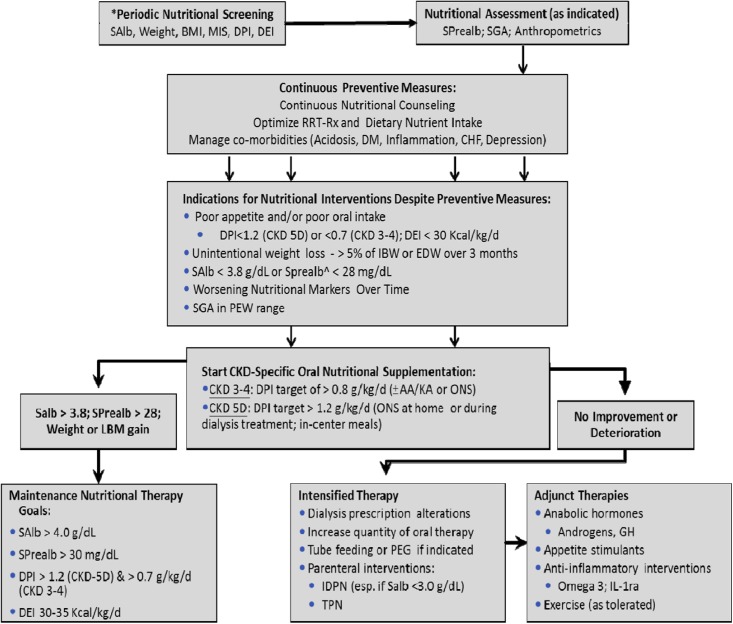
Protein energy wasting is common in patients with CKD and ESRD and is associated with adverse clinical outcomes, such as increased rates of hospitalization and death, in these patients. A multitude of factors can affect the nutritional and metabolic status of patients with CKD, including decreased dietary nutrient intake, catabolic effects of renal replacement therapy, systemic inflammation, metabolic and hormonal derangements, and comorbid conditions (such as diabetes and depression). Unique aspects of CKD also confound reliable assessment of nutritional status, further complicating management of this comorbid condition. In patients in whom preventive measures and oral dietary intake from regular meals cannot help them maintain adequate nutritional status, nutritional supplementation, administered orally, enterally, or parenterally, is effective in replenishing protein and energy stores. The advantages of oral nutritional supplements include proven efficacy, safety, and compliance. Anabolic steroids and exercise, with nutritional supplementation or alone, improve protein stores and represent potential additional approaches for the treatment of PEW. There are several emerging novel therapies, such as appetite stimulants, anti-inflammatory interventions, and anabolic agents.
Figures
References
-
- Fouque D, Kalantar-Zadeh K, Kopple J, Cano N, Chauveau P, Cuppari L, Franch H, Guarnieri G, Ikizler TA, Kaysen G, Lindholm B, Massy Z, Mitch W, Pineda E, Stenvinkel P, Treviño-Becerra A, Wanner C: A proposed nomenclature and diagnostic criteria for protein-energy wasting in acute and chronic kidney disease. Kidney Int 73: 391–398, 2008 - PubMed
-
- Ikizler TA, Hakim RM: Nutrition in end-stage renal disease. Kidney Int 50: 343–357, 1996 - PubMed
-
- Kalantar-Zadeh K, Block G, McAllister CJ, Humphreys MH, Kopple JD: Appetite and inflammation, nutrition, anemia, and clinical outcome in hemodialysis patients. Am J Clin Nutr 80: 299–307, 2004 - PubMed
-
- Clinical practice guidelines for nutrition in chronic renal failure. K/DOQI, National Kidney Foundation. Am J Kidney Dis 35: S1–140, 2000 - PubMed
-
- Jeejeebhoy KN: Nutritional assessment. Nutrition 16: 585–590, 2000 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
