

Safety of intracorporeal circular stapling esophagojejunostomy using trans-orally inserted anvil (OrVil) following laparoscopic total or proximal gastrectomy - comparison with extracorporeal anastomosis
- PMID: 23972079
- PMCID: PMC3765957
- DOI: 10.1186/1477-7819-11-209
Safety of intracorporeal circular stapling esophagojejunostomy using trans-orally inserted anvil (OrVil) following laparoscopic total or proximal gastrectomy - comparison with extracorporeal anastomosis
Abstract
Background: There have been several attempts to develop a unique and easier way to perform esophagojejunostomy during laparoscopy-assisted total gastrectomy or laparoscopy-assisted proximal gastrectomy. The OrVil system (Covidien, Mansfield, MA, USA) is one of those methods, but its technical and oncologic feasibility have not been proven and need to be observed.
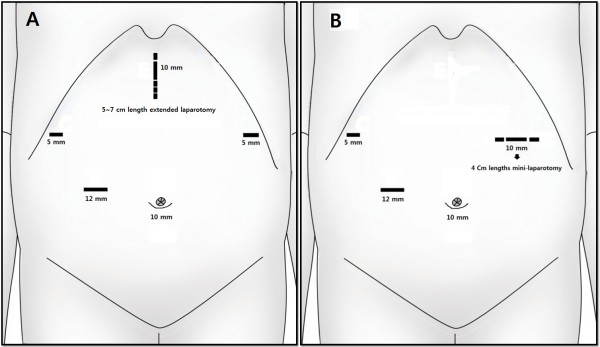
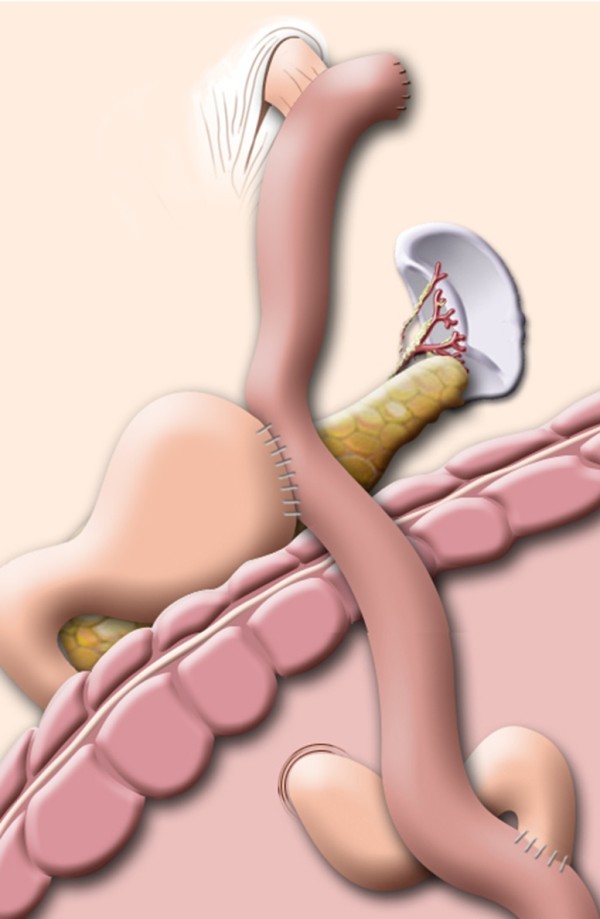
Methods: Among 87 patients who underwent laparoscopy-assisted total gastrectomy (LATG; 79 cases) and laparoscopy-assisted proximal gastrectomy with double tract anastomosis (LAPG_DT; 8 cases) from April 2004, 47 patients underwent the conventional extracorporeal method (Group I; 2004-2008) were compared with 40 patients treated with the intracorporeal OrVil system (Group II; 2009-2012).
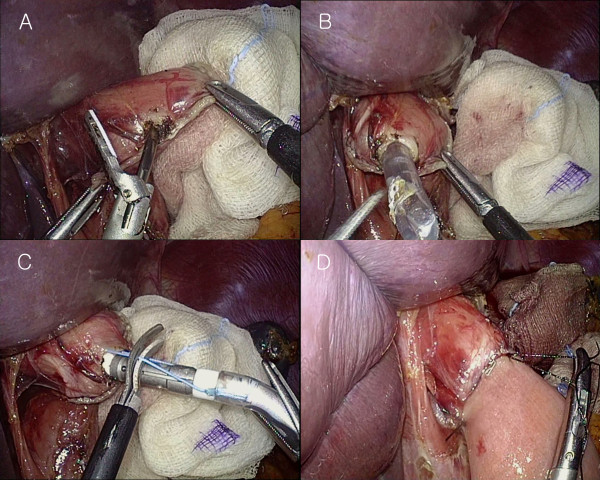
Results: There was no significant difference in clinicopathologic characteristics between the two groups except tumor location; more cardia lesions were involved in group II (p = 0.012). The mean time for esophagojejunostomy (E-J), defined as the time from anvil insertion to closure of the jejunal entry site has no significant difference (Group I vs II: 22.2 ± 3.2 min vs 18.6 ± 3.5 min, p = 0.623). In terms of anastomotic complication, there was no significant difference in E-J leakage and stricture. E-J leakage occurred in 2 out of 47 (4.3%) cases in group I and 2 out of 40 (5%) in group II (p = 0.628); half of them were treated conservatively in each group and the others underwent reoperation. E-J stricture occurred in 2 (4.3%) cases in group I and 1 (2.5%) in group II (p = 0.561), which required postoperative gastrofiberscopic balloon dilatation.
Conclusions: Esophagojejunostomy using the OrVil system was a feasible and safe technique compared with the conventional extracorporeal method through mini-laparotomy in terms of anastomotic complications. Moreover, it can help to reduce surgeon's stress regarding esophagojejunostomy because it needs no purse-string procedure and serves a secure operation view laparoscopically.
Figures
References
-
- Sakuramoto S, Yamashita K, Kikuchi S, Futawatari N, Katada N, Moriya H, Hirai K, Watanabe M. Clinical experience of laparoscopy-assisted proximal gastrectomy with Toupet-like partial fundoplication in early gastric cancer for preventing reflux esophagitis. J Am Coll Surg. 2009;11:344–351. doi: 10.1016/j.jamcollsurg.2009.04.011. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
