

Definition of compartment-based radical surgery in uterine cancer: radical hysterectomy in cervical cancer as 'total mesometrial resection (TMMR)' by M Höckel translated to robotic surgery (rTMMR)
- PMID: 23972128
- PMCID: PMC3765976
- DOI: 10.1186/1477-7819-11-211
Definition of compartment-based radical surgery in uterine cancer: radical hysterectomy in cervical cancer as 'total mesometrial resection (TMMR)' by M Höckel translated to robotic surgery (rTMMR)
Abstract
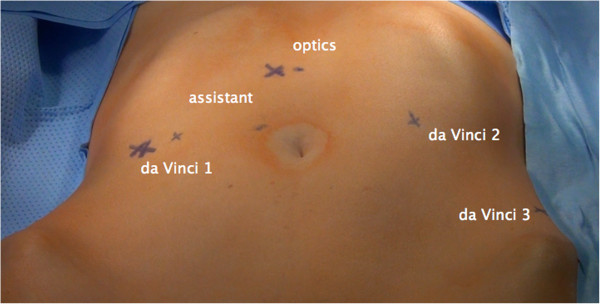
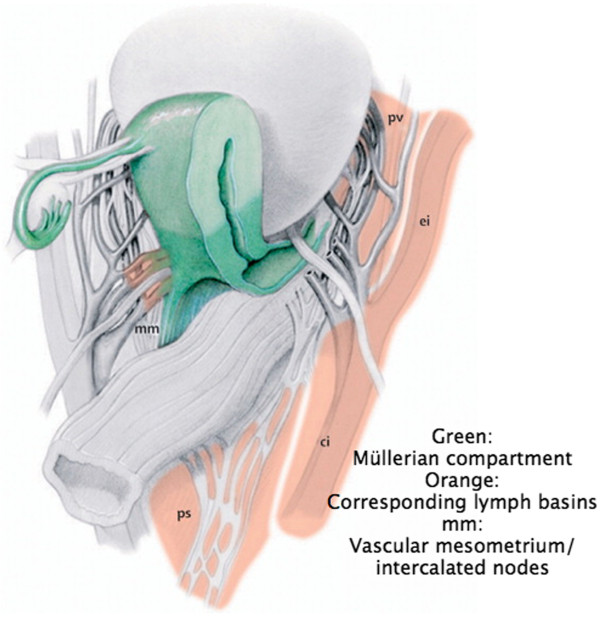
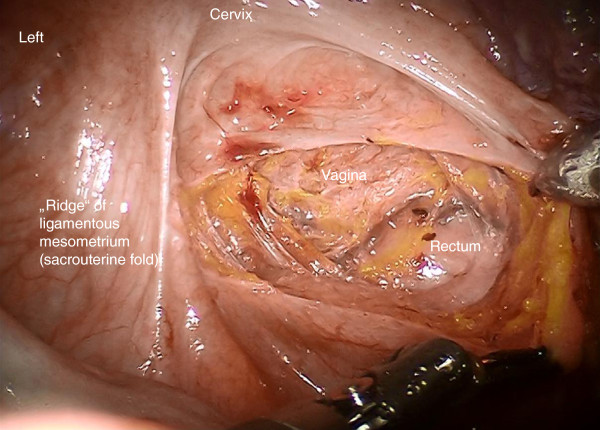
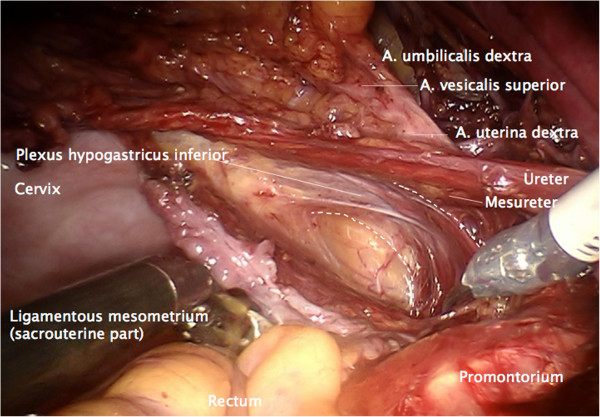
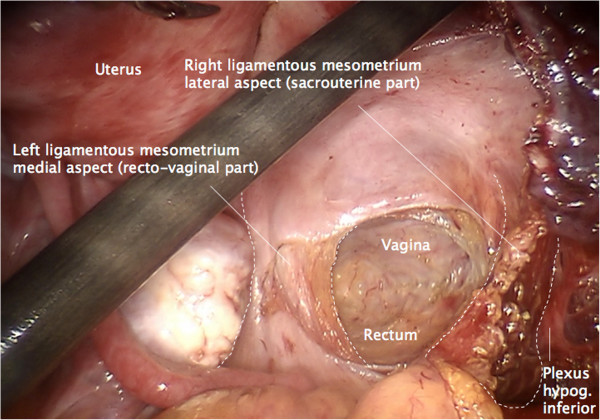
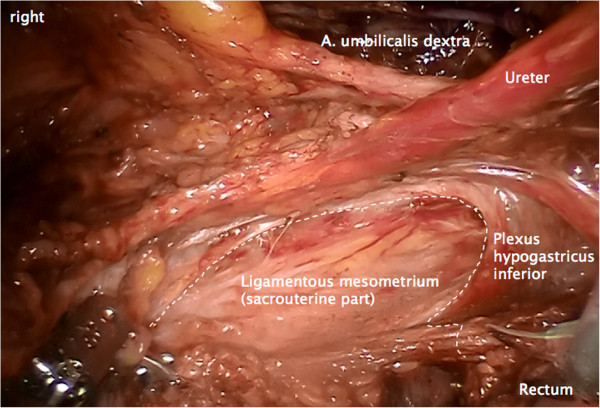
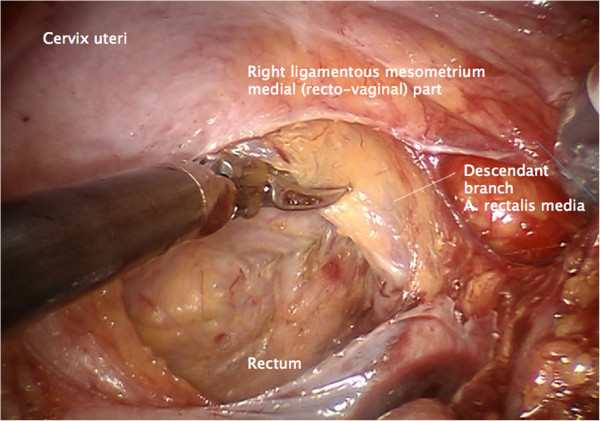
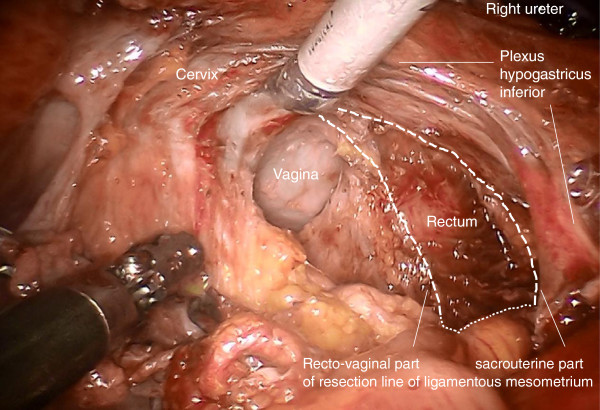
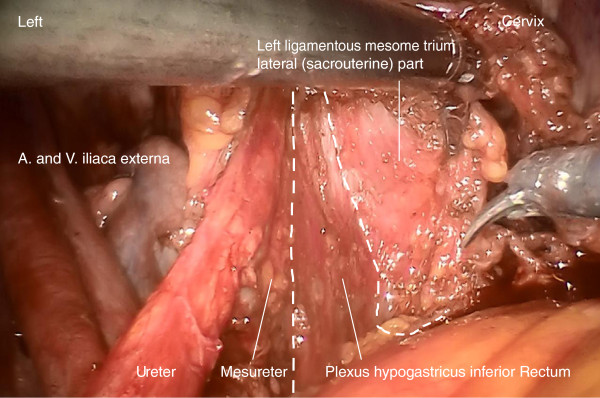
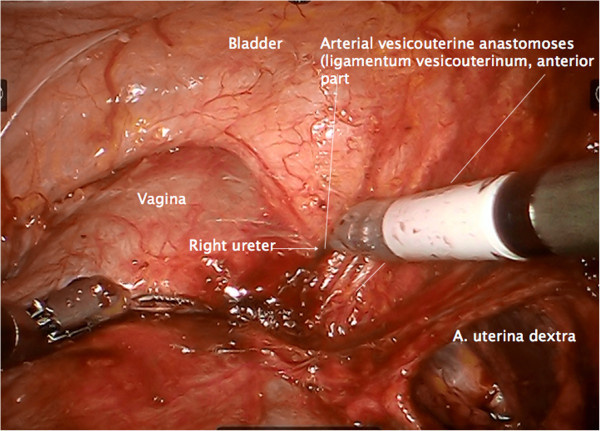
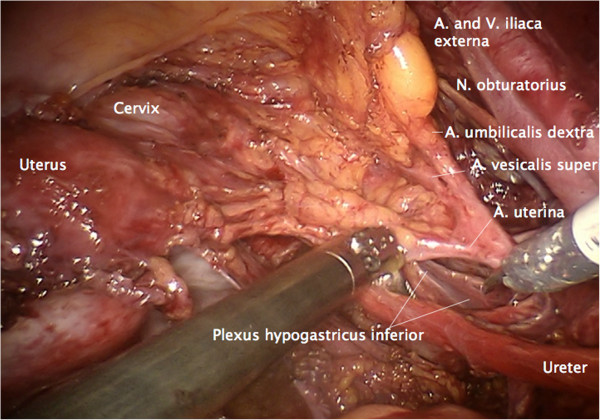
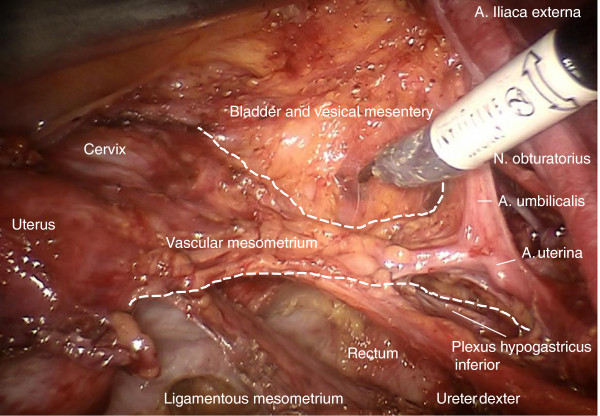
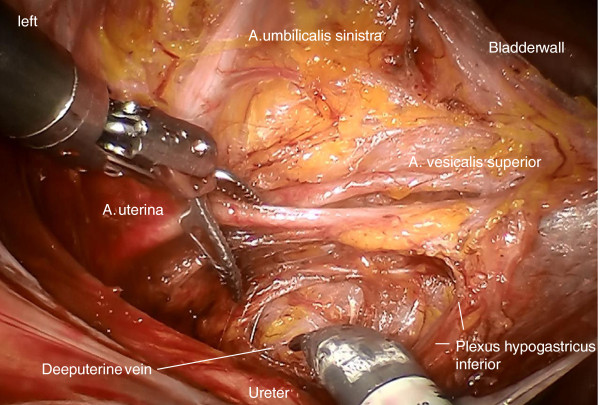
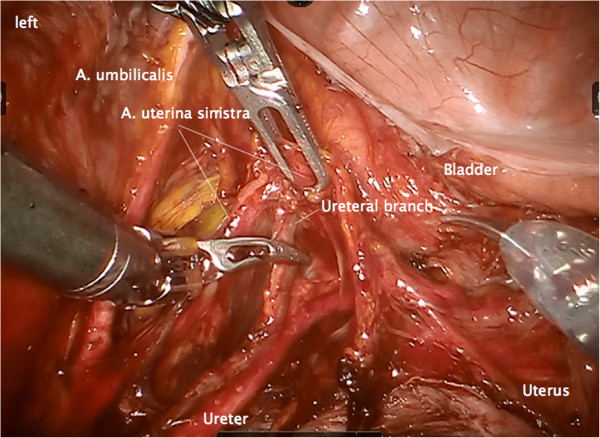
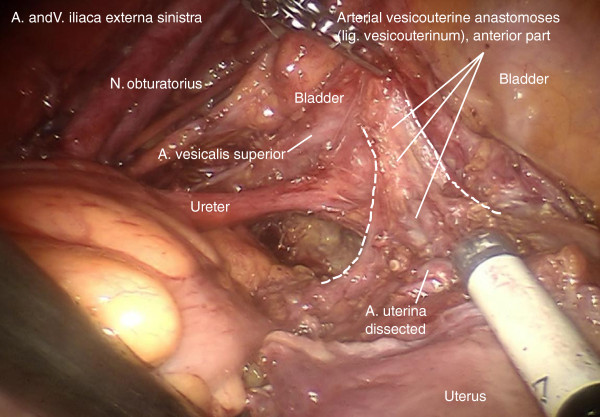
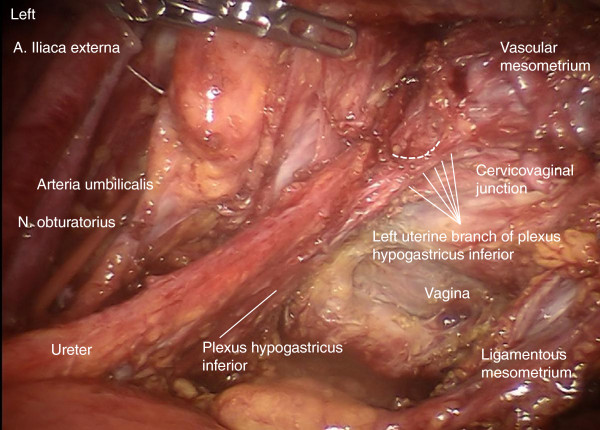
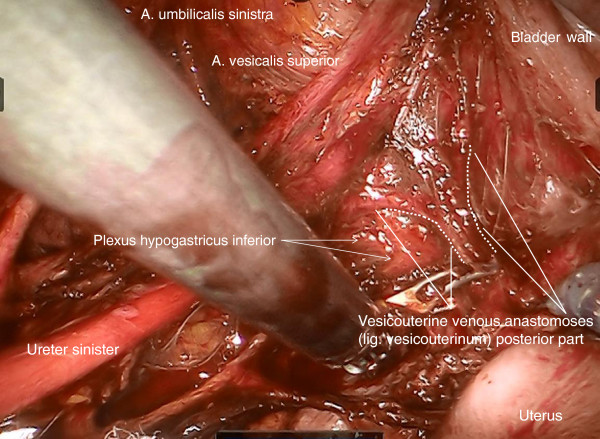
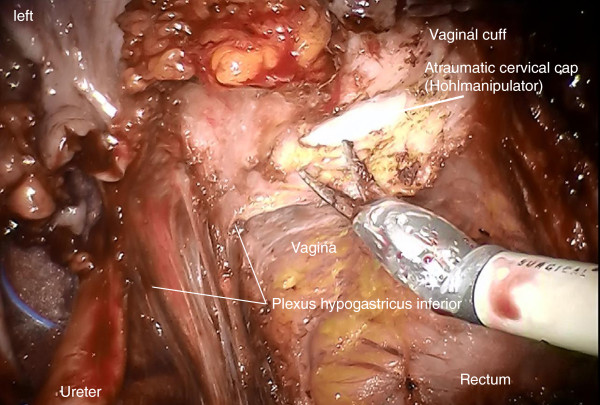
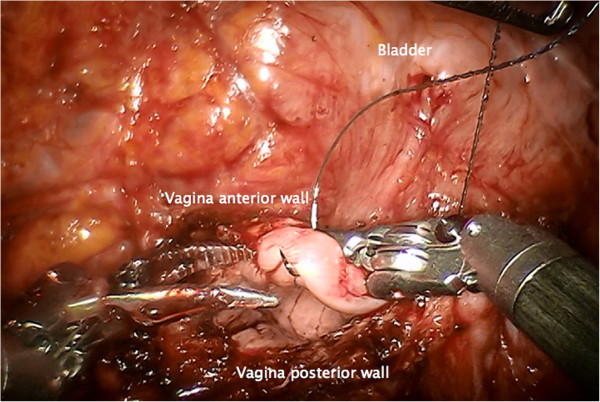
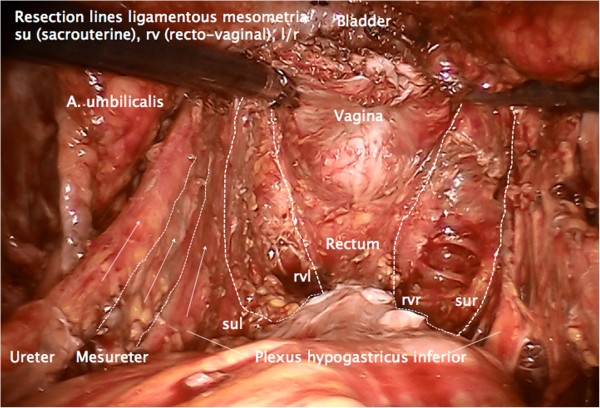
Background: Radical hysterectomy has been developed as a standard treatment in Stage I and II cervical cancers with and without adjuvant therapy. However, there have been several attempts to standardize the technique of radical hysterectomy required for different tumor extension with variable success. Total mesometrial resection as ontogenetic compartment-based oncologic surgery - developed by open surgery - can be standardized identically for all patients with locally defined tumors. It appears to be promising for patients in terms of radicalness as well as complication rates. Robotic surgery may additionally reduce morbidity compared to open surgery. We describe robotically assisted total mesometrial resection (rTMMR) step by step in cervical cancer and present feasibility data from 26 patients.
Methods: Patients (n = 26) with the diagnosis of cervical cancer were included. Patients were treated by robotic total mesometrial resection (rTMMR) and pelvic or pelvic/periaortic robotic therapeutic lymphadenectomy (rtLNE) for FIGO stage IA-IIB cervical cancer.
Results: No transition to open surgery was necessary. No intraoperative complications were noted. The postoperative complication rate was 23%. Within follow-up time (mean: 18 months) we noted one distant but no locoregional recurrence of cervical cancer. There were no deaths from cervical cancer during the observation period.
Conclusions: We conclude that rTMMR and rtLNE is a feasible and safe technique for the treatment of compartment-defined cervical cancer.
Figures
References
-
- Garcia-Bellido A, Ripoli P, Morata G. Developmental compartmentalization on the wing disk of Drosophila. Nat New Biol. 1973;11:251–253. - PubMed
-
- Dahmann C, Oates AC, Brand M. Boundary formation and maintenance in tissue development. Nature Reviews. 2011;11:43–55. - PubMed
-
- Quirke P, Dixon MF, Durdey P, Williams NS. Local recurrence of rectal adenocarcinoma due to inadequate surgical resection. Lancet. 1986;11:996–998. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
