

Adjuvant therapy in renal cell carcinoma-past, present, and future
- PMID: 23972712
- PMCID: PMC3765962
- DOI: 10.1053/j.seminoncol.2013.05.004
Adjuvant therapy in renal cell carcinoma-past, present, and future
Abstract
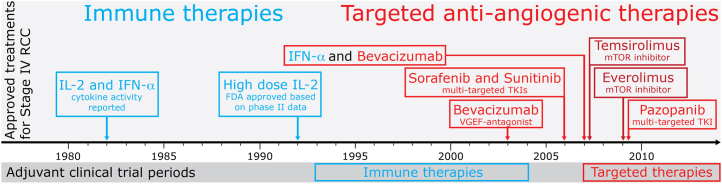
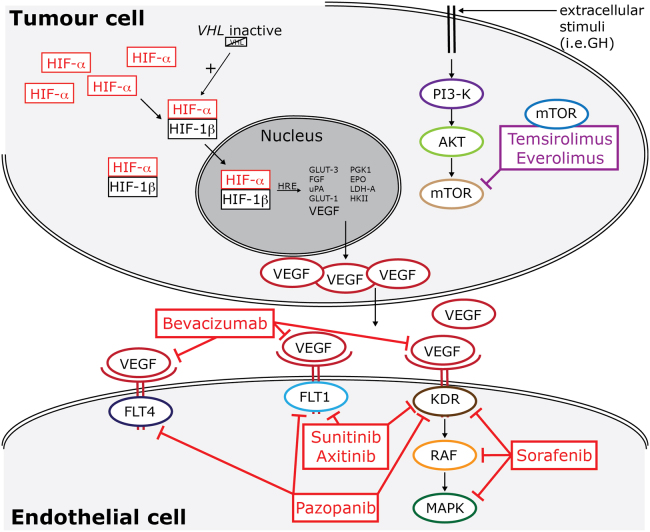
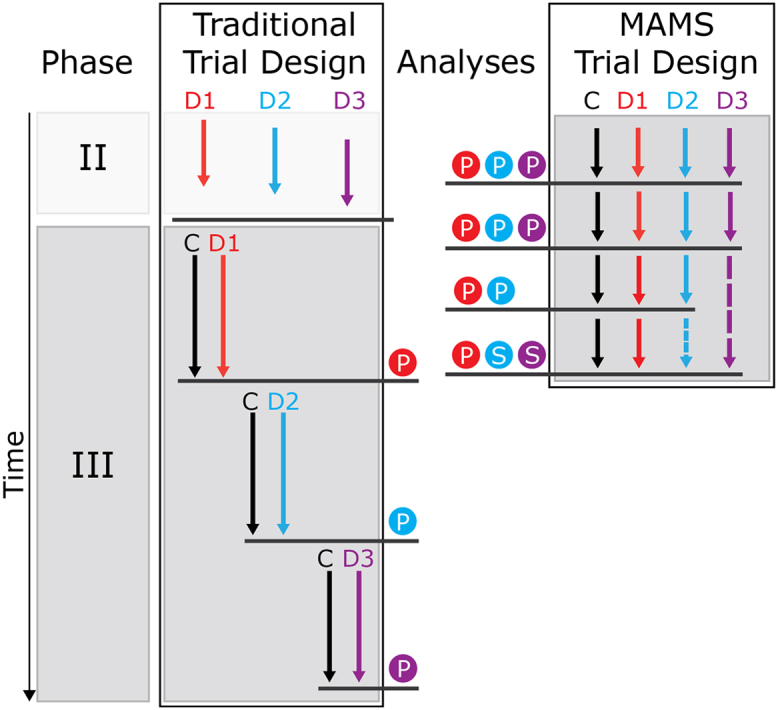
To date, no effective adjuvant treatment for renal cell carcinoma (RCC) has been described, but research in this area is important since the 5-year relapse rate for intermediate- and high-risk early-stage RCC is 30%-40%. Metastatic RCC can be treated successfully with immune therapy and targeted therapy. Adjuvant trials with immune therapy have been conducted, but they reported no benefit in disease-free survival, and clinical trials with targeted agents have not yet reported results. Further advances in our understanding of the molecular pathogenesis of RCC will identify additional potential targets for adjuvant treatment trials. Future challenges will consequently include target identification, as well as trial design to answer multiple trial questions concurrently, comprehensively, and economically. We review the past efforts, summarize the current adjuvant clinical trial landscape, and consider the challenges in adjuvant trials for RCC. Additionally, we identify potential future adjuvant trial treatments and propose an alternative design for future adjuvant clinical trials.
Crown Copyright © 2013 Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Ferlay J., Shin H.-R., Bray F., Forman D., Mathers C., Parkin D.M. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer. 2010;127(12):2893–2917. - PubMed
-
- Jemal A., Bray F., Center M.M., Ferlay J., Ward E., Forman D. Global cancer statistics. CA Cancer J Clin. 2011;61(2):69–90. - PubMed
-
- Chow W.H., Devesa S.S., Warren J.L., Fraumeni J.F. Rising incidence of renal cell cancer in the United States. JAMA. 1999;281(17):1628–1631. - PubMed
-
- Kane C.J., Mallin K., Ritchey J., Cooperberg M.R., Carroll P.R. Renal cell cancer stage migration: analysis of the National Cancer Data Base. Cancer. 2008;113(1):78–83. - PubMed
-
- Escudier B., Eisen T., Porta C. Renal cell carcinoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2012;23(suppl 7) vii65–vii71. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
