

Use of a web 2.0 portal to improve education and communication in young patients with families: randomized controlled trial
- PMID: 23973555
- PMCID: PMC3758041
- DOI: 10.2196/jmir.2425
Use of a web 2.0 portal to improve education and communication in young patients with families: randomized controlled trial
Abstract
Background: Diabetes requires extensive self-care and comprehensive knowledge, making patient education central to diabetes self-management. Web 2.0 systems have great potential to enhance health information and open new ways for patients and practitioners to communicate.
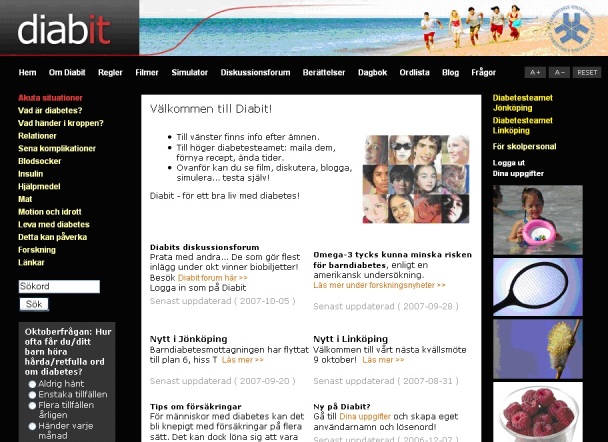
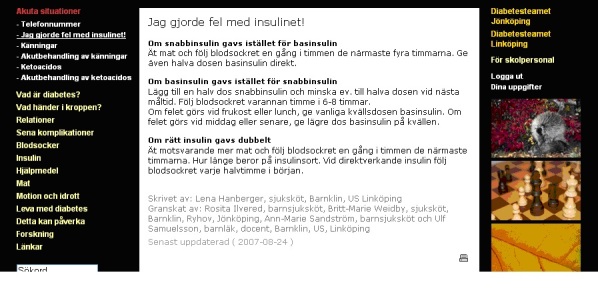
Objective: To develop a Web portal designed to facilitate self-management, including diabetes-related information and social networking functions, and to study its use and effects in pediatric patients with diabetes.
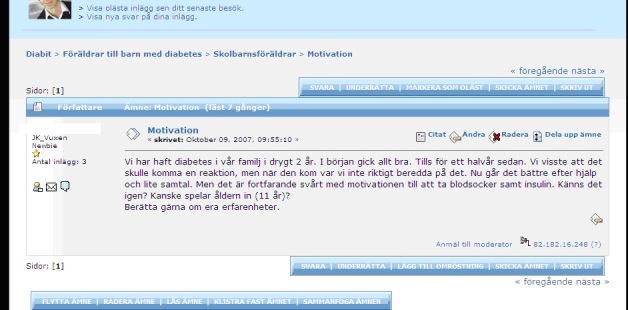
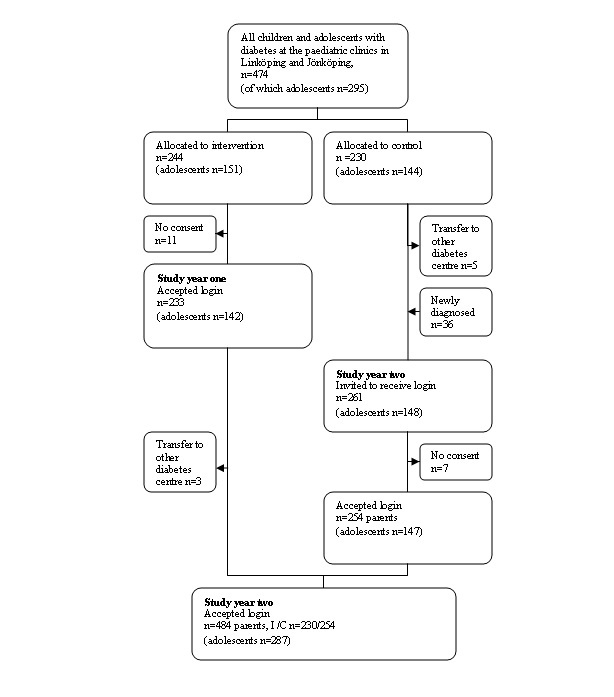
Methods: A Web 2.0 portal was developed in collaboration with patients, parents, and practitioners. It offered communication with local practitioners, interaction with peers, and access to relevant information and services. Children and adolescents with diabetes in a geographic population of two pediatric clinics in Sweden were randomized to a group receiving passwords for access to the portal or a control group with no access (n=230) for 1 year. All subjects had access during a second study year. Users' activity was logged by site and page visits. Health-related quality of life (HRQOL), empowerment (DES), and quality of information (QPP) questionnaires were given at baseline and after 1 and 2 study years. Clinical data came from the Swedish pediatric diabetes quality registry SWEDIABKIDS.
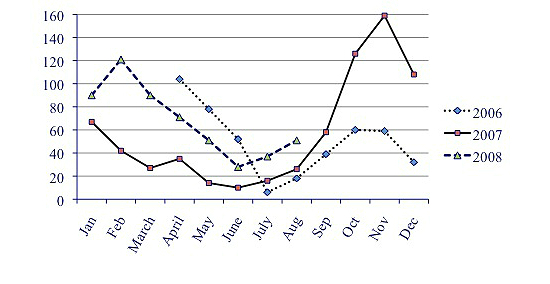
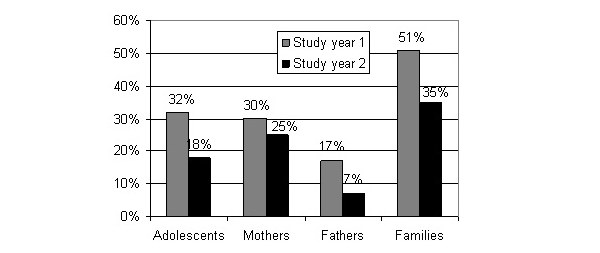
Results: There was a continuous flow of site visits, decreasing in summer and Christmas periods. In 119/233 families (51%), someone visited the portal the first study year and 169/484 (35%) the second study year. The outcome variables did not differ between intervention and control group. No adverse treatment or self-care effects were identified. A higher proportion of mothers compared to fathers visited once or more the first year (P<.001) and the second year (P<.001). The patients who had someone in the family visiting the portal 5 times or more, had shorter diabetes duration (P=.006), were younger (P=.008), had lower HbA1c after 1 year of access (P=.010), and were more often girls (P<.001). Peer interaction seems to be a valued aspect.
Conclusions: The Web 2.0 portal may be useful as a complement to traditional care for this target group. Widespread use of a portal would need integration in routine care and promotion by diabetes team members.
Trial registration: International Standard Randomized Controlled Trial Number (ISRCTN):92107365; http://www.controlled-trials.com/ISRCTN92107365/ (Archived by WebCite at http://webcitation.org/6IkiIvtSb).
Keywords: HbA1c; adolescent; children; health information technology; intervention studies; patient education; type 1 diabetes.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
References
-
- Graue M, Wentzel-Larsen T, Hanestad BR, Båtsvik B, Søvik O. Measuring self-reported, health-related, quality of life in adolescents with type 1 diabetes using both generic and disease-specific instruments. Acta Paediatr. 2003 Oct;92(10):1190–6. - PubMed
-
- Hoey H, Aanstoot HJ, Chiarelli F, Daneman D, Danne T, Dorchy H, Fitzgerald M, Garandeau P, Greene S, Holl R, Hougaard P, Kaprio E, Kocova M, Lynggaard H, Martul P, Matsuura N, McGee HM, Mortensen HB, Robertson K, Schoenle E, Sovik O, Swift P, Tsou RM, Vanelli M, Aman J. Good metabolic control is associated with better quality of life in 2,101 adolescents with type 1 diabetes. Diabetes Care. 2001 Nov;24(11):1923–8. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
