

Relationship of apolipoproteins A-1 and B, and lipoprotein(a) to cardiovascular outcomes: the AIM-HIGH trial (Atherothrombosis Intervention in Metabolic Syndrome with Low HDL/High Triglyceride and Impact on Global Health Outcomes)
- PMID: 23973688
- PMCID: PMC3800510
- DOI: 10.1016/j.jacc.2013.06.051
Relationship of apolipoproteins A-1 and B, and lipoprotein(a) to cardiovascular outcomes: the AIM-HIGH trial (Atherothrombosis Intervention in Metabolic Syndrome with Low HDL/High Triglyceride and Impact on Global Health Outcomes)
Abstract
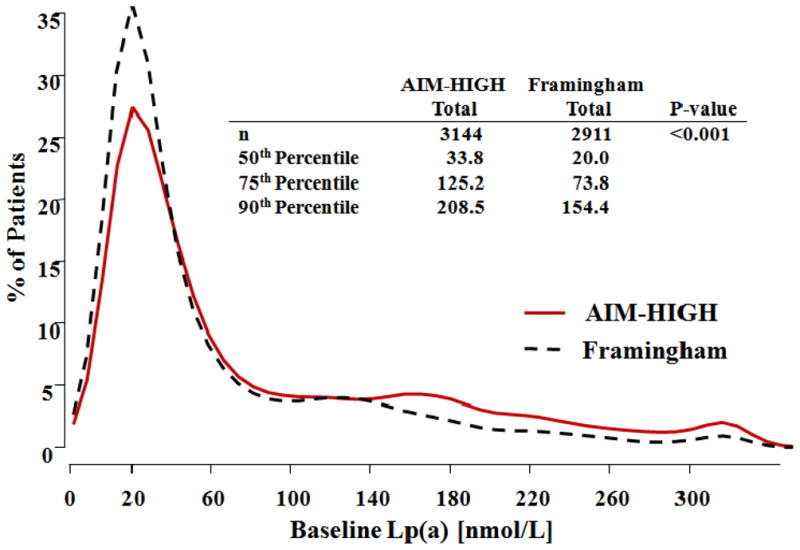
Objectives: This study sought to examine the relationship between baseline and on-study apolipoproteins (apo) A-1 and B and lipoprotein(a) [Lp(a)] levels and the development of subsequent cardiovascular (CV) events in the AIM-HIGH (Atherothrombosis Intervention in Metabolic Syndrome with Low HDL/High Triglyceride and Impact on Global Health Outcomes) trial.
Background: Niacin has been reported to lower apoB and Lp(a) and to raise apoA-1.
Methods: Individuals with CV disease and low baseline levels of high-density lipoprotein cholesterol were randomized to simvastatin plus placebo or simvastatin, plus extended-release niacin ([ERN], 1,500 to 2,000 mg/day), with ezetimibe added as needed, in both groups, to maintain an on-treatment low-density lipoprotein cholesterol in the range of 40 to 80 mg/dl. Hazard ratios (HRs) were used to evaluate the relationship between levels of apoA-1, apoB, and Lp(a), and CV events in each treatment group.
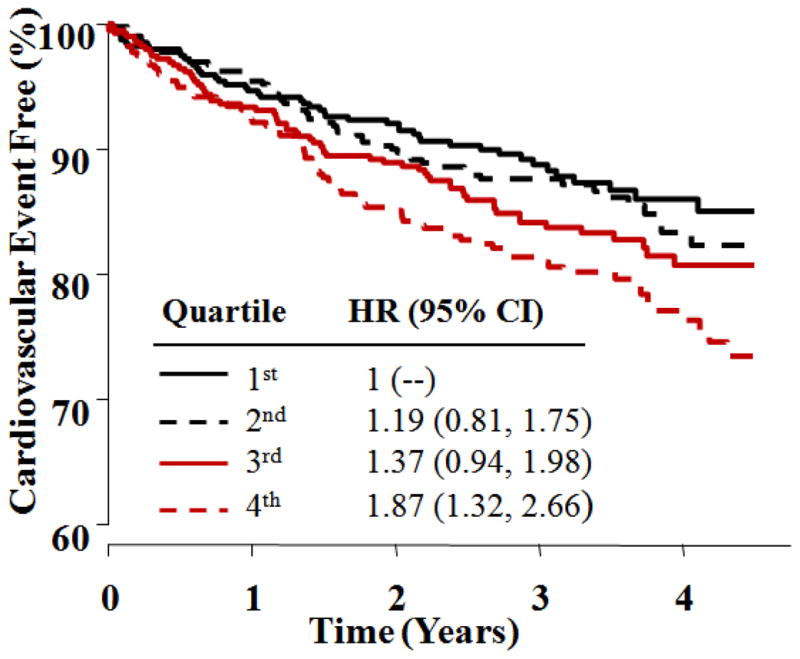
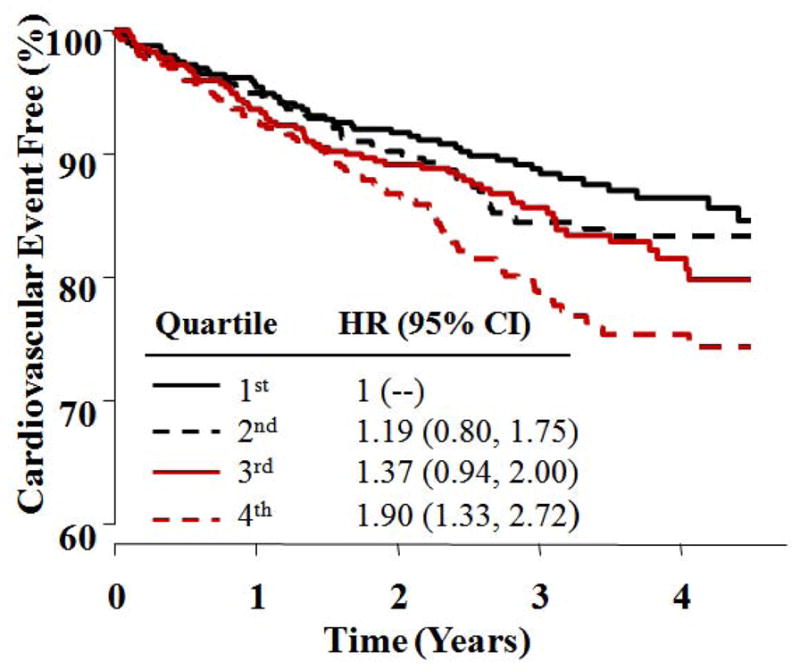
Results: Baseline apoB and the apoB/apoA-I ratio were significantly predictive of CV events only for the placebo group (HR: 1.17 [p = 0.018] and HR: 1.19 [p = 0.016]). Baseline and on-study Lp(a) were predictive of CV events in both simvastatin plus placebo (baseline HR: 1.24 [p = 0.002] and on-study HR: 1.21 [p = 0.017]) and the simvastatin plus ERN group (baseline HR: 1.25 [p = 0.001] and on-study HR: 1.18 [p = 0.028]). The ERN modestly increased 1-year apoA-1 (7%), decreased apoB (13%), decreased the ApoB/ApoA-1 ratio (19%), and decreased Lp(a) 21%, but did not reduce CV events.
Conclusions: Lp(a) was associated with increased CV risk in both treatment groups indicating that it contributes to residual CV risk. However, there was no evidence that ERN reduced CV risk, despite favorable lipoprotein changes.
Keywords: Apo; CV; ELISA; ERN; HDL-C; HR; LDL; LDL-C; Lp(a); apolipoprotein; apolipoproteins; cardiovascular; cardiovascular risk; enzyme-linked immunoadsorbent assay; extended-release niacin; hazard ratio; high-density lipoprotein cholesterol; lipoprotein(a); low-density lipoprotein; low-density lipoprotein cholesterol; niacin; simvastatin.
Copyright © 2013 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Boden WE, Probstfield JL, Anderson T, et al. The AIM-HIGH Investigators. Niacin in patients with Low HDL Cholesterol levels receiving intensive Statin therapy. N Engl J Med. 2011;365:2255–67. - PubMed
-
- Marcovina SM, Albers JJ, Gabel B, Koschinsky ML, Gaur VP. Effects of the number of apolipoprotein(a) kringle 4 domains on immunochemical measurement of lipoprotein(a) Clin Chem. 1995;41:246–55. - PubMed
-
- Maher VMG, Brown BG, Marcovina SM, et al. Effects of lowering elevated LDL cholesterol on the cardiovascular risk of lipoprotein(a) JAMA. 1995;274:1771–74. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
