

Cardiomyocyte injury assessed by a highly sensitive troponin assay and sudden cardiac death in the community: the Cardiovascular Health Study
- PMID: 23973690
- PMCID: PMC4157919
- DOI: 10.1016/j.jacc.2013.07.049
Cardiomyocyte injury assessed by a highly sensitive troponin assay and sudden cardiac death in the community: the Cardiovascular Health Study
Abstract
Objectives: This study sought to determine the association between markers of cardiomyocyte injury in ambulatory subjects and sudden cardiac death (SCD).
Background: The pathophysiology of SCD is complex but is believed to be associated with an abnormal cardiac substrate in most cases. The association between biomarkers of cardiomyocyte injury in ambulatory subjects and SCD has not been investigated.
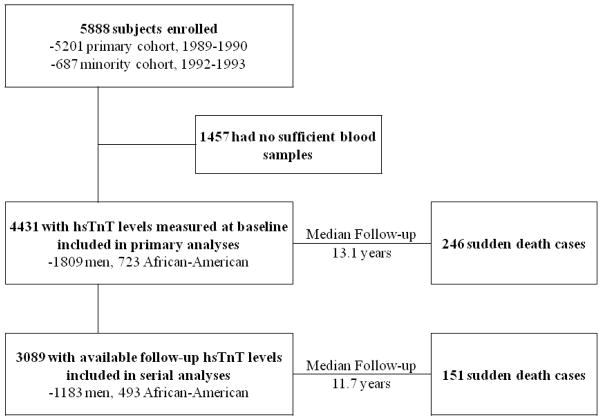
Methods: Levels of cardiac troponin T, a biomarker of cardiomyocyte injury, were measured by a highly sensitive assay (hsTnT) in 4,431 ambulatory participants in the Cardiovascular Health Study, a longitudinal community-based prospective cohort study. Serial measures were obtained in 3,089 subjects. All deaths, including SCD, were adjudicated by a central events committee.
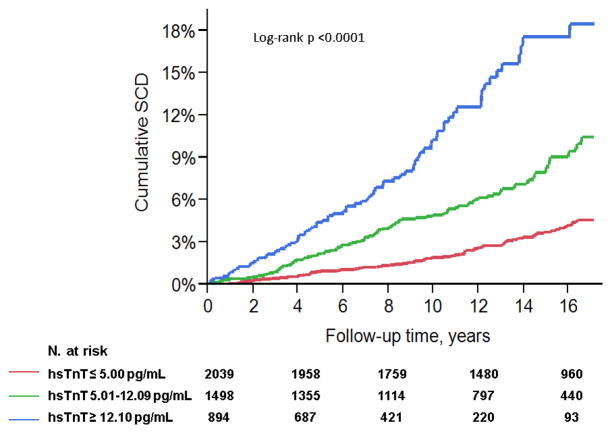
Results: Over a median follow-up of 13.1 years, 246 participants had SCD. Baseline levels of hsTnT were significantly associated with SCD (hazard ratio [HR] for +1 log(hsTnT): 2.04, 95% confidence interval [CI]: 1.78 to 2.34]. This association persisted in covariate-adjusted Cox analyses accounting for baseline risk factors (HR: 1.30, 95% CI: 1.05 to 1.62), as well as for incident heart failure and myocardial infarction (HR: 1.26, 95% CI: 1.01 to 1.57). The population was also categorized into 3 groups based on baseline hsTnT levels and SCD risk [fully adjusted HR: 1.89 vs. 1.55 vs. 1 (reference group) for hsTnT ≥12.10 vs. 5.01 to 12.09 vs. ≤ 5.00 pg/ml, respectively; p trend = 0.005]. On serial measurements, change in hsTnT levels was also associated with SCD risk (fully adjusted HR for +1 pg/ml per year increase from baseline: 1.03, 95% CI: 1.01 to 1.06).
Conclusions: The findings suggest an association between cardiomyocyte injury in ambulatory subjects and SCD risk beyond that of traditional risk factors.
Keywords: CI; HR; MI; SCD; cardiac troponin T levels by a highly sensitive assay; confidence interval(s); general population; hazard ratio(s); hsTnT; myocardial infarction; myocytes; sudden cardiac death; sudden death.
Copyright © 2013 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures

Comment in
-
Highly sensitive troponin assay and sudden cardiac death in the community: unlocking the pathophysiology of sudden cardiac death one biomarker at a time.J Am Coll Cardiol. 2013 Dec 3;62(22):2121-3. doi: 10.1016/j.jacc.2013.07.048. Epub 2013 Aug 21. J Am Coll Cardiol. 2013. PMID: 23973705 No abstract available.
References
-
- Ford ES, Ajani UA, Croft JB, et al. Explaining the decrease in U.S. deaths from coronary disease, 1980–2000. N Engl J Med. 2007;356:2388–98. - PubMed
-
- Rosamond WD, Chambless LE, Folsom AR, et al. Trends in the incidence of myocardial infarction and in mortality due to coronary heart disease, 1987 to 1994. N Engl J Med. 1998;339:861–7. - PubMed
-
- Fox CS, Evans JC, Larson MG, Kannel WB, Levy D. Temporal trends in coronary heart disease mortality and sudden cardiac death from 1950 to 1999: The framingham heart study. Circulation. 2004;110:522–7. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- N01 HC085086/HC/NHLBI NIH HHS/United States
- N01-HC-85081/HC/NHLBI NIH HHS/United States
- R56 AG020098/AG/NIA NIH HHS/United States
- AG-20098/AG/NIA NIH HHS/United States
- N01-HC-85086/HC/NHLBI NIH HHS/United States
- AG-027058/AG/NIA NIH HHS/United States
- N01 HC085080/HC/NHLBI NIH HHS/United States
- HHSN268201200036C/HL/NHLBI NIH HHS/United States
- N01 HC055222/HL/NHLBI NIH HHS/United States
- N01-HC-55222/HC/NHLBI NIH HHS/United States
- R01 HL080295/HL/NHLBI NIH HHS/United States
- R01 AG020098/AG/NIA NIH HHS/United States
- N01-HC-85079/HC/NHLBI NIH HHS/United States
- HL080295/HL/NHLBI NIH HHS/United States
- R01 AG027058/AG/NIA NIH HHS/United States
- N01-HC-85084/HC/NHLBI NIH HHS/United States
- N01 HC085081/HC/NHLBI NIH HHS/United States
- N01-HC-85085/HC/NHLBI NIH HHS/United States
- R01 AG015928/AG/NIA NIH HHS/United States
- U01 HL080295/HL/NHLBI NIH HHS/United States
- HHSN268200800007C/HL/NHLBI NIH HHS/United States
- N01 HC085086/HL/NHLBI NIH HHS/United States
- N01 HC085083/HC/NHLBI NIH HHS/United States
- N01 HC085082/HC/NHLBI NIH HHS/United States
- N01-HC-85082/HC/NHLBI NIH HHS/United States
- N01 HC085079/HL/NHLBI NIH HHS/United States
- N01-HC-85083/HC/NHLBI NIH HHS/United States
- N01-HC-75150/HC/NHLBI NIH HHS/United States
- N01-HC-85080/HC/NHLBI NIH HHS/United States
- N01-HC-85239/HC/NHLBI NIH HHS/United States
- AG-023629/AG/NIA NIH HHS/United States
- N01 HC085079/HC/NHLBI NIH HHS/United States
- N01 HC075150/HL/NHLBI NIH HHS/United States
- R01 AG023629/AG/NIA NIH HHS/United States
- N01 HC035129/HC/NHLBI NIH HHS/United States
- R56 AG023629/AG/NIA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
