

Beyond medication prescription as performance measures: optimal secondary prevention medication dosing after acute myocardial infarction
- PMID: 23973701
- PMCID: PMC3819453
- DOI: 10.1016/j.jacc.2013.04.102
Beyond medication prescription as performance measures: optimal secondary prevention medication dosing after acute myocardial infarction
Erratum in
- J Am Coll Cardiol. 2014 Mar 11;63(9):944
Abstract
Objectives: The aim of this study was to examine the prescribing patterns of medications quantified by the performance measures for acute myocardial infarction (AMI).
Background: Current performance measures for AMI are designed to improve quality by quantifying the use of evidence-based treatments. However, these measures only assess medication prescription. Whether patients receive optimal dosing of secondary prevention medications at the time of and after discharge after AMI is unknown.
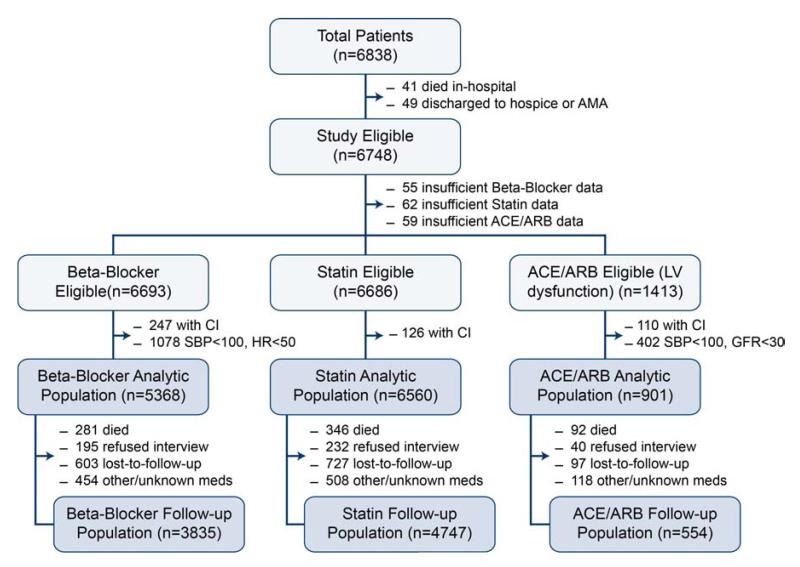
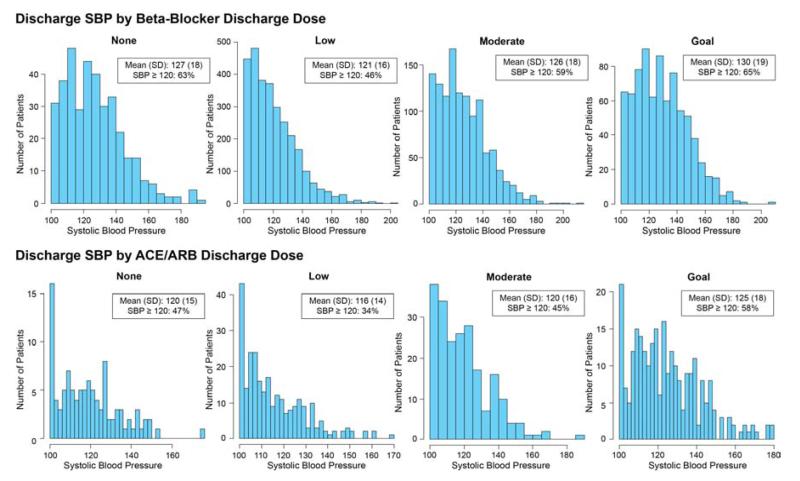
Methods: We assessed treatment doses of beta-blockers, statins, and angiotensin-converting enzyme inhibitors (ACEI)/angiotensin II receptor blockers (ARBs) at discharge and 12 months after AMI among 6,748 patients from 31 hospitals enrolled in 2 U.S. registries (2003 to 2008). Prescribed doses were categorized as none, low (<50% target [defined from seminal clinical trials]), moderate (50% to 74% target), or goal (≥ 75% target). Patients with contraindications were excluded from analyses for that medication.
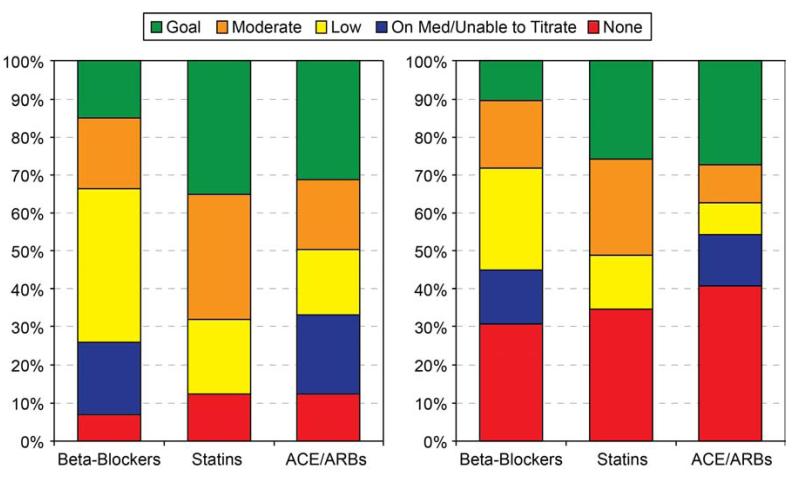
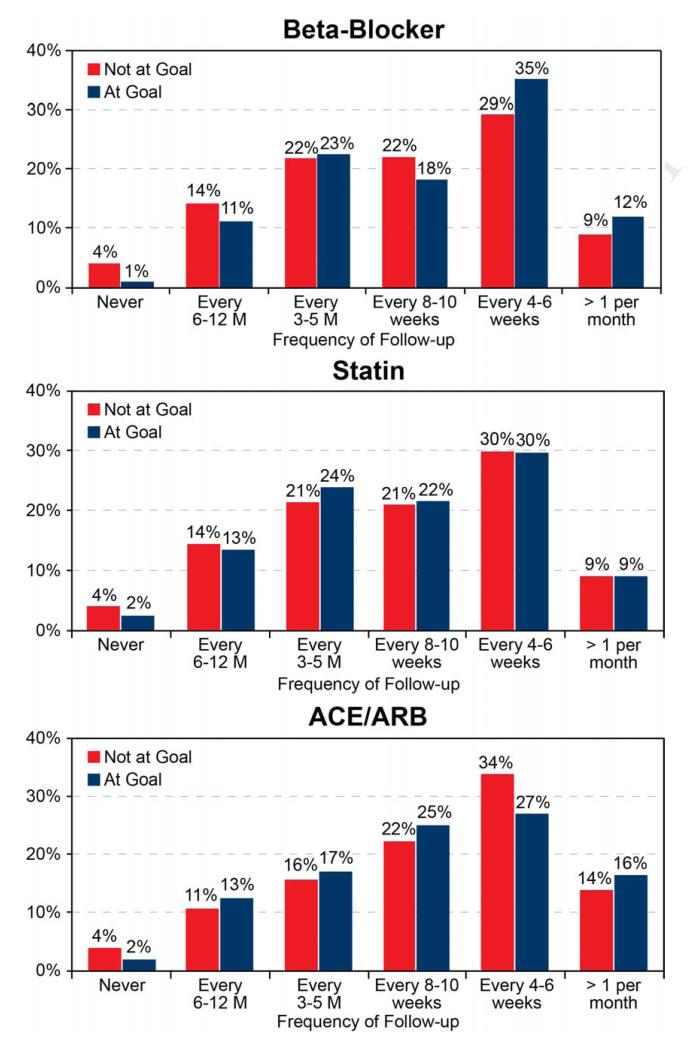
Results: Most eligible patients (>87%) were prescribed some dose of each medication at discharge, although only 1 in 3 patients were prescribed these medications at goal doses. Of patients not discharged on goal doses, up-titration during follow-up occurred infrequently (approximately 25% of patients for each medication). At 12 months, goal doses of beta-blockers, statins, and ACEI/ARBs were achieved in only 12%, 26%, and 32% of eligible patients, respectively. After multivariable adjustment, prescription of goal dose at discharge was strongly associated with being at goal dose at follow-up: beta-blockers, adjusted odds ratio (OR): 6.08 (95% confidence interval [CI]: 3.70 to 10.01); statins, adjusted OR: 8.22 (95% CI: 6.20 to 10.90); ACEI/ARBs, adjusted OR: 5.80 (95% CI: 2.56 to 13.16); p < 0.001 for each.
Conclusions: Although nearly all patients after an AMI are discharged on appropriate secondary prevention medications, dose increases occur infrequently, and most patients are prescribed doses below those with proven efficacy in clinical trials. Integration of dose intensity into performance measures might help improve the use of optimal medical therapy after AMI.
Keywords: ACEI; AMI; ARB; CI; LDL-C; LV; OR; SBP; acute myocardial infarction; angiotensin II receptor blocker; angiotensin-converting enzyme inhibitor; confidence interval; left ventricular; low-density lipoprotein cholesterol; myocardial infarction; odds ratio; performance measures; secondary prevention; systolic blood pressure.
Copyright © 2013 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Should we measure quality by the dose?J Am Coll Cardiol. 2013 Nov 5;62(19):1802-3. doi: 10.1016/j.jacc.2013.07.059. Epub 2013 Aug 21. J Am Coll Cardiol. 2013. PMID: 23973702 No abstract available.
References
-
- Krumholz HM, Anderson JL, Bachelder BL, et al. ACC/AHA 2008 performance measures for adults with ST-elevation and non-ST-elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Performance Measures (Writing Committee to develop performance measures for ST-elevation and non-ST-elevation myocardial infarction): developed in collaboration with the American Academy of Family Physicians and the American College of Emergency Physicians: endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation, Society for Cardiovascular Angiography and Interventions, and Society of Hospital Medicine. Circulation. 2008;118:2596–648. - PubMed
-
- Peterson ED, Roe MT, Mulgund J, et al. Association between hospital process performance and outcomes among patients with acute coronary syndromes. JAMA. 2006;295:1912–20. - PubMed
-
- Bristow MR, Gilbert EM, Abraham WT, et al. MOCHA Investigators Carvedilol produces dose-related improvements in left ventricular function and survival in subjects with chronic heart failure. Circulation. 1996;94:2807–16. - PubMed
-
- Svanström H, Pasternak B, Hviid A. Association of treatment with losartan vs candesartan and mortality among patients with heart failure. JAMA. 2012;307:1506–12. - PubMed
-
- Packer M, Poole-Wilson PA, Armstrong PW, et al. ATLAS Study Group Comparative effects of low and high doses of the angiotensin-converting enzyme inhibitor, lisinopril, on morbidity and mortality in chronic heart failure. Circulation. 1999;100:2312–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
