

The spectrum of achalasia: lessons from studies of pathophysiology and high-resolution manometry
- PMID: 23973923
- PMCID: PMC3835179
- DOI: 10.1053/j.gastro.2013.08.038
The spectrum of achalasia: lessons from studies of pathophysiology and high-resolution manometry
Abstract
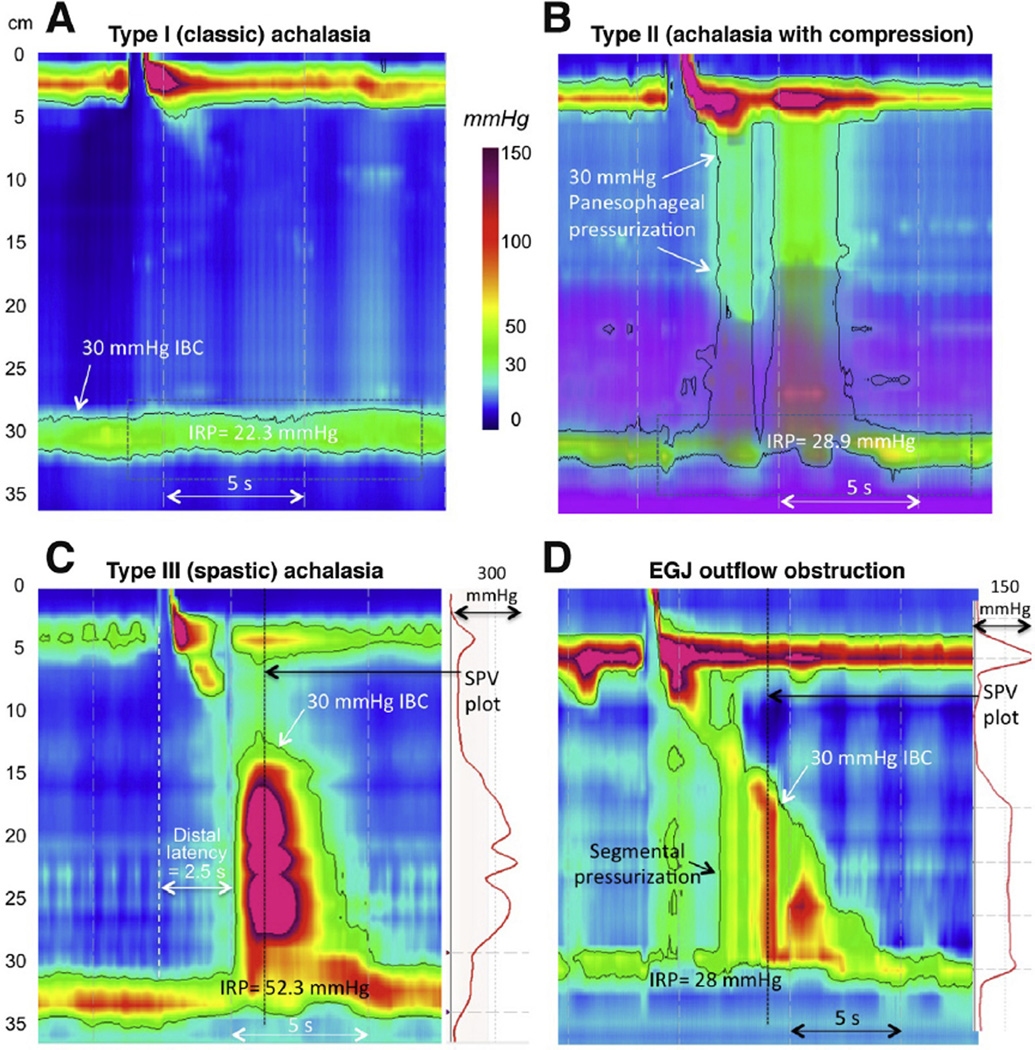
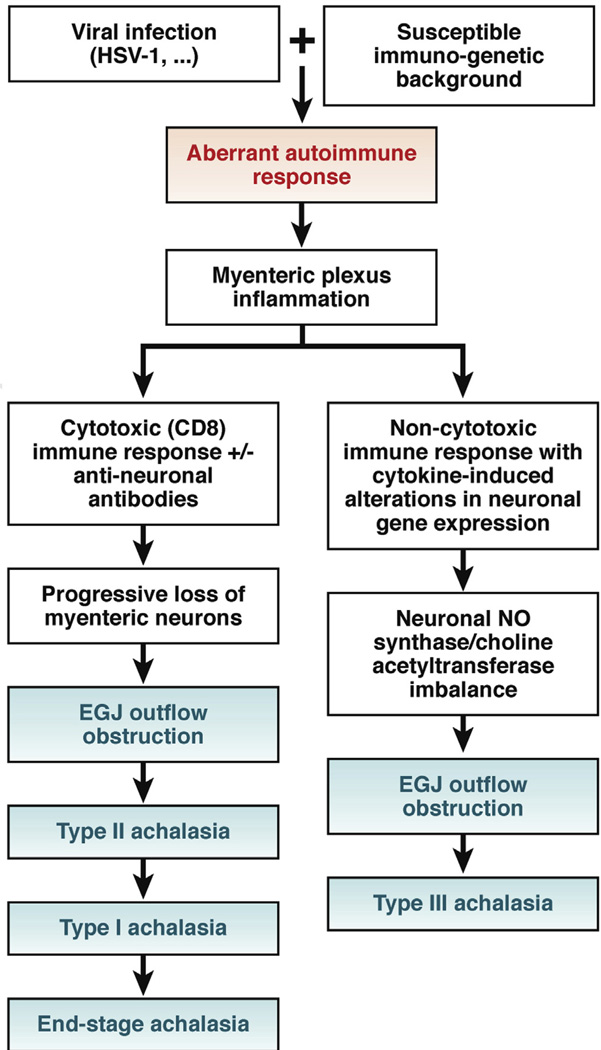
High-resolution manometry and recently described analysis algorithms, summarized in the Chicago Classification, have increased the recognition of achalasia. It has become apparent that the cardinal feature of achalasia, impaired lower esophageal sphincter relaxation, can occur in several disease phenotypes: without peristalsis, with premature (spastic) distal esophageal contractions, with panesophageal pressurization, or with peristalsis. Any of these phenotypes could indicate achalasia; however, without a disease-specific biomarker, no manometric pattern is absolutely specific. Laboratory studies indicate that achalasia is an autoimmune disease in which esophageal myenteric neurons are attacked in a cell-mediated and antibody-mediated immune response against an uncertain antigen. This autoimmune response could be related to infection of genetically predisposed subjects with herpes simplex virus 1, although there is substantial heterogeneity among patients. At one end of the spectrum is complete aganglionosis in patients with end-stage or fulminant disease. At the opposite extreme is type III (spastic) achalasia, which has no demonstrated neuronal loss but only impaired inhibitory postganglionic neuron function; it is often associated with accentuated contractility and could be mediated by cytokine-induced alterations in gene expression. Distinct from these extremes is progressive plexopathy, which likely arises from achalasia with preserved peristalsis and then develops into type II achalasia and then type I achalasia. Variations in its extent and rate of progression are likely related to the intensity of the cytotoxic T-cell assault on the myenteric plexus. Moving forward, we need to integrate the knowledge we have gained into treatment paradigms that are specific for individual phenotypes of achalasia and away from the one-size-fits-all approach.
Keywords: Achalasia; Dysphagia; EGJ; EPT; Esophageal Motility; HSV-1; IRP; LES; Pathogenesis; TLESR; esophageal pressure topography; esophagogastric junction; herpes simplex virus 1; integrated relaxation pressure; lower esophageal sphincter; transient lower esophageal sphincter relaxation.
Copyright © 2013 AGA Institute. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflicts of interest
The authors disclose no conflicts.
Figures
References
-
- Lendrum FC. Anatomic features of the cardiac orifice of the stomach with special reference to cardiospasm. Arch Intern Med. 1937;59:474–451.
-
- Pandolfino JE, Kahrilas PJ. The second American Gastroenterological Association technical review on the clinical use of esophageal manometry. Gastroenterology. 2005;128:209–229. - PubMed
-
- Pandolfino JE, Kahrilas PJ. American Gastroenterological Association medical position statement: clinical use of esophageal manometry. Gastroenterology. 2005;128:207–208. - PubMed
-
- Kahrilas PJ, Kishk SM, Helm JF, et al. A comparison of pseudoachalasia and achalasia. Am J Med. 1987;82:439–446. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
